

EXTERNAL GENITAL ORGANS (SYN: VULVA, PUDENDUM)
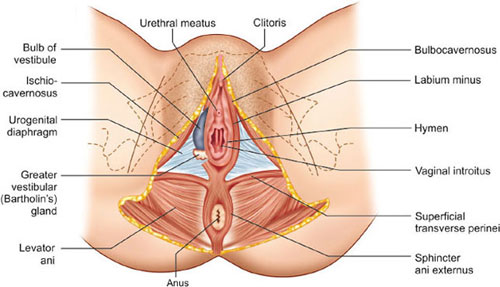
The vulva includes mons veneris, labia majora, labia minora, clitoris, vestibule and conventionally the perineum. These are all visible on external examination. It is, therefore, bounded anteriorly by the mons veneris, laterally by the labia majora and posteriorly by the perineum (Fig. 1.1).
MONS VENERIS (MONS PUBIS)
It is the pad of subcutaneous adipose connective tissue lying in front of the pubis and, in the adult female, is covered by hair.
LABIA MAJORA
The vulva is bounded on each side by the elevation of skin and subcutaneous tissue, which form the labia majora. They are continuous where they join medially to form the posterior commissure in front of the anus. The inner surface of the labia majora are hairless. The labia majora are covered with squamous epithelium and contain sebaceous glands, sweat glands and hair follicles. Beneath the skin, there are dense connective tissue and adipose tissue. The adipose tissue is richly supplied by venous plexus, which may produce hematoma, if injured during childbirth. The labia majora are homologous with the scrotum in the male. The round ligaments terminate at its anterior third.
LABIA MINORA
Labia minora are two thick folds of skin, devoid of fat, on either side just within the labia majora. Except in the parous women, they are only exposed when the labia majora are separated. Anteriorly, they are divided to enclose the clitoris and unite with each other in front and behind the clitoris to form the prepuce and frenulum, respectively. The lower portion of the labia minora fuses across the midline to form a fold of skin known as fourchette. It is usually injured during childbirth. Between the fourchette and the vaginal orifice is the fossa navicularis. The labia minora do not contain hair follicle. The folds contain connective tissues, numerous sebaceous glands, erectile muscle fibers and numerous vessels and nerve endings. It is homologous to the ventral aspect of the penis.
CLITORIS
Clitoris is a small cylindrical erectile body, measuring about 2.5 cm situated in the most anterior part of the vulva. It consists of glans, a body and two crura. The glans is covered by squamous epithelium and is richly supplied with nerves. The vessels of the clitoris are connected with the vestibular bulb and are liable to be injured during childbirth. Clitoris is an analog to the penis in the male, but it differs basically in being entirely separate from the urethra. It is attached to the undersurface of the symphysis pubis by the suspensory ligament.
VESTIBULE
Vestibule is a triangular space bounded anteriorly by the clitoris, posteriorly by the fourchette and on either side by labium minus. There are four openings into the vestibule (Fig. 1.1).
Urethral Opening
The opening is situated in the midline, just in front of the vaginal orifice about 1–1.5 cm below the pubic arch. The paraurethral ducts open either on the posterior wall of the urethral orifice or directly into the vestibule.
Vaginal Orifice and Hymen
The vaginal orifice lies in the posterior end of the vestibule and is of varying size and shape. In virgins and nulliparae, the opening is closed by the labia minora but in parous, it may be exposed. It is incompletely closed by a septum of mucous membrane, called hymen. The membrane varies in shape but is usually circular or crescentic in virgins. The hymen is usually ruptured at the consummation of marriage.2


During childbirth, the hymen is extremely lacerated and is later represented by cicatrized nodules of varying sizes, called the carunculae myrtiformes. On both sides, it is lined by stratified squamous epithelium.
BARTHOLIN'S GLAND
The Bartholin's glands are situated in the superficial perineal pouch, close to the posterior end of the vestibular bulb. They are pea-sized, of about 0.5 cm and yellowish-white in color. During sexual excitement, it secretes abundant alkaline mucus which helps in lubrication. Contraction of bulbocavernosus helps squeeze the secretion. The glands are compound racemose variety and are lined by columnar epithelium. Each gland has got a duct which measures about 2 cm and opens into the vestibule, outside the hymen at the junction of the anterior two-thirds and posterior one-third in the groove between the hymen and the labium minus. The duct is lined by columnar epithelium but near its opening by stratified squamous epithelium (Fig. 1.2). The Bartholin's gland corresponds to the bulbourethral gland of male.

Vestibular Bulbs
These are bilateral elongated masses of erectile tissues situated beneath the mucous membrane of the vestibule. Each bulb lies on either side of the vaginal orifice in front of the Bartholin's gland and is incorporated within the bulbocavernosus muscles. They are homologous to the single bulb of the penis and corpus spongiosum in the male. They are likely to be injured during childbirth with brisk hemorrhage (Fig. 1.3).
PERINEUM
The details of the anatomy of perineum are described later in this Chapter (p. ).
BLOOD SUPPLY OF THE VULVA
Arteries: (a) Branches of internal pudendal artery—the chief being labial, transverse perineal, artery to the vestibular bulb and deep and dorsal arteries to the clitoris and (b) branches of femoral artery—superficial and deep pudendal.
Veins: The veins form plexuses and drain into—(a) Internal pudendal vein; (b) Vesical or vaginal venous plexus; (c) Long saphenous vein. Varicosities during pregnancy are not uncommon and may rupture spontaneously causing visible bleeding or hematoma formation.
NERVE SUPPLY OF THE VULVA
The supply is through bilateral spinal somatic nerves. Anterosuperior part is supplied by the cutaneous branches from the ilioinguinal and genital branch of genitofemoral nerve (L1 and L2) and the posteroinferior part by the pudendal branches from the posterior cutaneous nerve of thigh (S2,3,4). Between these two groups, the vulva is supplied by the labial and perineal branches of the pudendal nerve (S2,3,4).
INTERNAL GENITAL ORGANS
The internal genital organs in female include vagina, uterus, fallopian tubes, and the ovaries. These organs are placed internally and require special instruments for inspection.
VAGINA
The vagina is a fibromusculomembranous sheath com-municating the uterine cavity with the exterior at the vulva. It constitutes the excretory channel for the uterine secretion and menstrual blood. It is the organ of copulation and forms the birth canal of parturition. The canal is directed upwards and backwards forming an angle of 45° with the horizontal in erect posture. The long axis of the vagina almost lies parallel to the plane of the pelvic inlet and at right angle to that of the uterus. The diameter of the canal is about 2.5 cm, being the widest in the upper part and the narrowest at its introitus. It has got enough power of distensibility as evident during childbirth.
Walls
Vagina has got an anterior, a posterior, and two lateral walls. The anterior and posterior walls are apposed together but the lateral walls are comparatively stiffer especially at its middle, as such it looks ‘H’ shaped on transverse section. The length of the anterior wall is about 7 cm and that of the posterior wall is about 9 cm (Figs. 1.4A and B). The upper end of vagina is above the pelvic floor.
Fornices
The fornices are the clefts formed at the top of vagina (vault) due to the projection of the uterine cervix through the anterior vaginal wall, where it is blended inseparably with its wall. There are four fornices—one anterior, one posterior, and two lateral; the posterior one being deeper and the anterior, most shallow one.
Relations
Anterior: The upper one-third is related with base of the bladder and the lower two-thirds are with the urethra, the lower half of which is firmly embedded with its wall (Figs. 1.4A and B).
Posterior: The upper one-third is related with the pouch of Douglas, the middle-third with the anterior rectal wall separated by rectovaginal septum, and the lower-third is separated from the anal canal by the perineal body (Fig. 1.5).
Lateral walls: The upper one-third is related with the pelvic cellular tissue at the base of broad ligament in which the ureter and the uterine artery lie approximately 2 cm from the lateral fornices. The middle-third is blended with the levator ani and the lower-third is related with the bulbocavernosus muscles, vestibular bulbs, and Bartholin's glands (Fig. 1.6).
Structures
Layers from within outwards are: (a) Mucous coat which is lined by stratified squamous epithelium without any secreting glands; (b) Submucous layer of loose areolar vascular tissues; (c) Muscular layer consisting of indistinct inner circular and outer longitudinal and; (d) Fibrous coat derived from the endopelvic fascia which is tough and highly vascular (Fig. 1.7).

Figs. 1.4A and B: (A) Relation of the anterior and posterior vaginal wall; (B) ‘H’ shaped on cross-section.

Fig. 1.5: Mid-sagittal section of the female pelvis showing relative positions of the pelvic organs.


Epithelium
The vaginal epithelium is under the action of sex hormones (Fig. 1.8). At birth and up to 10–14 days, the epithelium is stratified squamous under the influence of maternal estrogen circulating in the newborn. Thereafter, up to prepuberty and in postmenopause, the epithelium becomes thin, consisting of few layers only.
From puberty till menopause, the vaginal epithelium is stratified squamous and devoid of any gland. Three distinct layers are defined—basal cells, intermediate cells, and superficial cornified cells. The intermediate and superficial cells contain glycogen under the influence of estrogen. These cells become continuous with those covering the vaginal portion of the cervix and extend up to the squamocolumnar junction at the external os. The superficial cells exfoliate constantly and more so in inflammatory or neoplastic condition. Replacement of the superficial cells occurs from the basal cells. When the epithelium is exposed to the dry external atmosphere, keratinization occurs. Unlike skin, it does not contain hair follicle, sweat, and sebaceous gland.5

Secretion
The vaginal secretion is very small in amount, sufficient to make the surface moist. Normally, it may be little excess in mid-menstrual or just prior to menstruation, during pregnancy, and during sexual excitement. The secretion is mainly derived from the glands of the cervix, uterus, transudation of the vaginal epithelium, and Bartholin's glands (during sexual excitement).
The pH is acidic and varies during different phases of life and menstrual cycle. Conversion of glycogen in the exfoliated squamous cells to lactic acid by the Doderlein's bacilli is dependent on estrogen. As such, the pH is more towards acidic during childbearing period and ranges between 4 and 5.5 with average of 4.5. The pH is highest in upper vagina because of contaminated cervical secretion (alkaline). The vaginal secretion consists of tissue fluid, epithelial debris, some leukocytes (never contains more than an occasional pus cell), electrolytes, proteins, and lactic acid (in a concentration of 0.75%). Apart from Doderlein's bacilli, it contains many pathogenic organism including Clostridium welchii. The glycogen content is highest in the vaginal fornix to the extent of 2.5–3 mg% and is lowest in the lower-third being 0.6–0.9 mg%.
Doderlein's bacillus: It is a rod-shaped gram-positive bacillus which grows anaerobically on acid media. It appears in the vagina 3–4 days after birth and disappears after 10–14 days. It appears again at puberty and disappears after menopause. It probably comes from the intestine. Its presence is dependent on estrogen, and its function is to convert the glycogen present in the vaginal mucosa into lactic acid so that the vaginal pH is maintained towards acidic side. This acidic pH prevents growth of the other pathogenic organisms (Fig. 1.8).
Blood Supply
The arteries involved are: (a) Cervicovaginal branch of the uterine artery; (b) Vaginal artery—a branch of anterior division of internal iliac or in common origin with the uterine; (c) Middle rectal; (d) Internal pudendal. These anastomose with one another and form two azygos arteries—anterior and posterior.
Veins drain into internal iliac and internal pudendal veins.
Nerve Supply
The vagina is supplied by sympathetic and parasympa-thetic nerves from the pelvic plexus. The lower part is supplied by the pudendal nerve.
UTERUS
The uterus is a hollow pyriform muscular organ situated in the pelvis between the bladder in front and the rectum behind (Fig. 1.5).6
Position
Its normal position is one of the anteversion and anteflexion. The uterus usually inclines to the right (dextrorotation) so that the cervix is directed to the left (levorotation) and comes in close relation with the left ureter.
Measurements and Parts
The uterus measures about 8 cm long, 5 cm wide at the fundus and its walls are about 1.25 cm thick. Its weight varies from 50–80 g. It has got the following parts (Fig. 1.9).
- Body or corpus
- Isthmus
- Cervix
Body or corpus: The body is further divided into fundus—the part which lies above the openings of the uterine tubes. The body properly is triangular and lies between the openings of the tubes and the isthmus. The superolateral angles of the body of the uterus project outwards from the junction of the fundus and body and are called the cornua of the uterus. The uterine tube, round ligament, and ligament of the ovary are attached to each cornu.
Isthmus: The isthmus is a constricted part measuring about 0.5 cm situated between the body and the cervix. It is limited above by the anatomical internal os and below by the histological internal os (Aschoff). Some consider isthmus as a part of the lower portion of the body of the uterus.
Cervix: The cervix is the lowermost part of the uterus. It extends from the histological internal os and ends at external os which opens into the vagina after perforating the anterior vaginal wall. It is almost cylindrical in shape and measures about 2.5 cm in length and diameter. It is divided into a supravaginal part—the part lying above the vagina and a vaginal part which lies within the vagina, each measuring 1.25 cm. In nulliparous, the vaginal part of the cervix is conical with the external os looking circular, whereas in parous, it is cylindrical with the external os having bilateral slits. The slit is due to invariable tear of the circular muscles surrounding the external os and gives rise to anterior and posterior lips of the cervix.

Cavity
The cavity of the uterine body is triangular on coronal section with the base above and the apex below. It measures about 3.5 cm. There is no cavity in the fundus. The cervical canal is fusiform and measures about 2.5 cm. Thus, the normal length of the uterine cavity including the cervical canal is usually 6–7 cm (Fig. 1.9).
Relations
Anteriorly: Above the internal os, the body forms the posterior wall of the uterovesical pouch. Below the internal os, it is separated from the base of the bladder by loose areolar tissue (Fig. 1.10).
Posteriorly: It is covered by peritoneum and forms the anterior wall of the pouch of Douglas containing coils of intestine (Fig. 1.10).
Laterally: The double folds of peritoneum of the broad ligament are attached laterally between which the uterine artery ascends up. Attachment of the Mackenrodt's ligament extends from the internal os down to the supravaginal cervix and lateral vaginal wall. About 1.5 cm away at the level of internal os, a little nearer on the left side is the crossing of the uterine artery and the ureter. The uterine artery crosses from above and in front of the ureter, soon before the ureter enters the ureteric tunnel (Fig. 1.11).
Structures
Body
The wall consists of three layers from outside inwards:
- Perimetrium: It is the serous coat which invests the entire organ except on the lateral borders. The peritoneum is intimately adherent to the underlying muscles.
- Myometrium: It consists of thick bundles of smooth muscle fibers held by connective tissues and are arranged in various directions. During pregnancy, however, three distinct layers can be identified—outer longitudinal, middle interlacing, and inner circular.
- Endometrium: The mucous lining of the cavity is called endometrium. As there is no submucous layer, the endometrium is directly apposed to the muscle coat.It consists of lamina propria and surface epithelium. The surface epithelium is a single layer of ciliated columnar epithelium. The lamina propria contains stromal cells, endometrial glands, vessels and nerves. The glands are simple tubular and lined by mucus secreting non-ciliated columnar epithelium which penetrate the stroma and sometimes even enter the muscle coat. All the components are changed during menstrual cycles (Ch. 8). The endometrium is changed to decidua during pregnancy.


Cervix
The cervix is composed mainly of fibrous connective tissues. The smooth muscle fibers average 10–15%. Only the posterior surface has got peritoneal coat (Fig. 1.5).
Epithelial lining of the cervix
Endocervical canal and glands: There is a median ridge on both the anterior and posterior surface of the canal from which transverse folds radiate. This arrangement is called arbor vitae uteri. The canal is lined by single layer of tall columnar epithelium with basal nuclei. Those placed over the top of the folds are ciliated. There are patches of cubical basal or reserve cells underneath the columnar epithelium. These cells may undergo squamous metaplasia or may replace the superficial cells.
The glands which dip into the stroma are of complex racemose type and are lined by secretory columnar epithelium. There is no stroma unlike the corpus and the lining epithelium rests on a thin basement membrane. The change in the epithelium and the glands during menstrual cycle and pregnancy are not so much as those in the endometrium.
Portio vaginalis: It is covered by stratified squamous epithelium and extends right up to the external os where there is abrupt change to columnar type.
The transitional zone (transformation zone) may be of 1–10 mm width with variable histological features. The zone consists of endocervical stroma and glands covered by squamous epithelium. The zone is not static but changes with hormone level of estrogen. The site is constantly irritated not only by hormones but also by infection and trauma. Thus, there is more chance of severe dysplasia, carcinoma in situ or even invasive carcinoma at this zone (Fig. 1.12) (p. 269).
Secretion: The endometrial secretion is scanty and watery. The physical and chemical properties of the cervical secretion change with menstrual cycle and with pregnancy. The cervical glands secrete an alkaline mucus with pH 7.8. The mucus is rich in fructose, glycoprotein, and mucopolysaccharides. It also contains sodium chloride. The fructose has got nutritive function to the spermatozoa. Under estrogenic stimulation, glycoprotein network is arranged parallel to each other thus facilitating sperm ascent. Progesterone produces interlacing bridges thereby preventing sperm penetration. Cervical mucus contributes significantly to the normal vaginal discharge. A part forms the mucus plug which functionally closes the cervical canal and has got bacteriolytic property.

Pelvic Peritoneum in Relation to the Uterus
This is described later in the chapter.
Blood Supply
Arterial supply: The arterial supply is from the uterine artery—one on each side. The artery arises directly from the anterior division of the internal iliac or in common with superior vesical artery. The other sources are ovarian and vaginal arteries to which the uterine arteries anastomose. The uterine artery crosses the ureter anteriorly about 1.5 cm away at the level of internal os before it ascends up along the lateral border of the uterus in between the leaves of broad ligament. The internal blood supply of the uterus is shown in Figure 2.1.
Nerve Supply
The nerve supply of the uterus is derived principally from the sympathetic system and partly from the parasympathetic system. Sympathetic components are from T5 and T6 (motor) and T10 to L1 spinal segments (sensory). The somatic distribution of uterine pain is that area of the abdomen supplied by T10 to L1. The parasympathetic system is represented on either side by the pelvic nerve which consists of both motor and sensory fibers from S2, S3, S4 and ends in the ganglia of Frankenhauser which lies on either sides of the cervix.
The cervix is insensitive to touch, heat and also when it is grasped by any instrument. The uterus, too is insensitive to handling and even to incision over its wall.
Changes of Uterus with Age
At birth, the uterus lies in the false pelvis; the cervix is much longer than the body. In childhood, the proportion is maintained but reduced to 2:1. At puberty, the body is growing faster under the action of ovarian steroids (estrogens) and the proportion is reversed to 1:2 and following childbirth, it becomes even 1:3. After menopause the uterus atrophies; the overall length is reduced; the walls become thinner, less muscular but more fibrous (Figs. 5.1A to E).
Position of the Uterus
The normal position of the uterus is anteversion and anteflexion. Anteversion relates the long axis of the cervix to the long axis of vagina which is about 90°. Anteflexion relates the long axis of the body to the long axis of the cervix and is about 120°. In about 15–20%, normally the uterus remains in retroverted position. In erect posture, the internal os lies on the upper border of the symphysis pubis and the external os lies at the level of ischial spines.
FALLOPIAN TUBE (SYN: UTERINE TUBE)
The uterine tubes are paired structures, measuring about 10 cm (4”) and are situated in the medial three-fourth of the upper free margin of the broad ligaments. Each tube has got two openings, one communicating with the lateral angle of the uterine cavity, called uterine opening and measures 1 mm in diameter, the other is on the lateral end of the tube, called pelvic opening or abdominal ostium and measures about 2 mm in diameter (Fig. 1.13).
Parts: There are four parts, from medial to lateral, they are—(1) Intramural or interstitial lying in the uterine wall and measures 1.25 cm (1/2”) in length and 1 mm in diameter; (2) Isthmus almost straight and measures about 2.5 cm (1”) in length and 2.5 mm in diameter; (3) Ampulla—tortuous part and measures about 5 cm (2”) in length which ends in wide; (4) Infundibulum measuring about 1.25 cm (1/2”) long with a maximum diameter of 6 mm. The abdominal ostium is surrounded by a number of radiating fimbriae, one of these is longer than the rest and is attached to the outer pole of the ovary called ovarian fimbria (Fig. 1.14).
Structures—it consists of three layers:
- Serous: Consists of peritoneum on all sides except along the line of attachment of mesosalpinx.
- Muscular: Arranged in two layers—outer longitudinal and inner circular.
- Mucous membrane is thrown into longitudinal folds. It is lined by columnar epithelium, partly ciliated, others secretory nonciliated and ‘Peg cells’. The epithelium rests on delicate vascular reticulum of connective tissue. There is no submucous layer nor any glands. Changes occur in the tubal epithelium during menstrual cycle but are less pronounced and there is no shedding (Fig. 1.14).
Functions: The important functions of the tubes are— (1) Transport of gametes; (2) To facilitate fertilization; (3) Survival of zygote through its secretion.
Blood supply: Arterial supply is from the uterine and ovarian. Venous drainage is through the pampiniform plexus into the ovarian veins.
Nerve supply: The nerve supply is derived from the uterine and ovarian nerves. The tube is very much sensitive to handling.
OVARY
The ovaries are paired sex glands or gonads in female which are concerned with:
- Germ cell maturation, storage and its release
- Steroidogenesis.

Fig. 1.13: Half of uterine cavity and fallopian tube of one side are cut open to show different parts of the tube. The vestigial structures in the broad ligament are shown.

Each gland is oval in shape and pinkish-gray in color and the surface is scarred during reproductive period. It measures about 3 cm in length, 2 cm in breadth and 1 cm in thickness. Each ovary presents two ends—tubal and uterine, two borders—mesovarium and free posterior and two surfaces—medial and lateral.
The ovaries are intraperitoneal structures. In nulliparae, the ovary lies in the ovarian fossa on the lateral pelvic wall. The ovary is attached to the posterior layer of the broad ligament by the mesovarium, to the lateral pelvic wall by infundibulopelvic ligament and to the uterus by the ovarian ligament.
Relations: Mesovarium or anterior border—a fold of peritoneum from the posterior leaf of the broad ligament is attached to the anterior border through which the ovarian vessels and nerves enter the hilum of the gland. Posterior border is free and is related with tubal ampulla. It is separated by the peritoneum from the ureter and the internal iliac artery. Medial surface is related to fimbrial part of the tube. Lateral surface is in contact with the ovarian fossa on the lateral pelvic wall.
The ovarian fossa is related superiorly to the external iliac vein, posteriorly to ureter and internal iliac vessels and laterally to the peritoneum separating the obturator vessels and nerves (Fig. 1.15).
Structures
The ovary is covered by a single layer of cubical cell known as germinal epithelium.


It is a misnomer as germ cells are not derived from this layer. The substance of the gland consists of outer cortex and inner medulla (Fig. 1.16).
Cortex: It consists of stromal cells which are thickened beneath the germinal epithelium to form tunica albuginea. During reproductive period (i.e. from puberty to menopause), the cortex is studded with numerous follicular structures, called the functional units of the ovary in various phases of their development. These are related to sex hormone production and ovulation. The structures include primordial follicles, maturing follicles, Graafian follicles and corpus luteum. Atresia of the structures results in formation of atretic follicles or corpus albicans (Fig. 1.16). The structural changes during ovular cycle are described in Chapter 8 (p. ).
Medulla: It consists of loose connective tissues, few unstriped muscles, blood vessels, and nerves. There are small collection of cells called “hilus cells” which are homologous to the interstitial cells of the testes.
Blood Supply
Arterial supply is from the ovarian artery, a branch of the abdominal aorta.
Venous drainage is through pampiniform plexus, that forms the ovarian veins which drain into inferior vena cava on the right side and left renal vein on the left side. Part of the venous blood from the placental site drains into the ovarian and thus may become the site of thrombophlebitis in puerperium.
Nerve Supply
Sympathetic supply comes down along the ovarian artery from T10 segment. Ovaries are sensitive to manual squeezing.
FEMALE URETHRA
The female urethra extends from the neck of the bladder to the external urethral meatus. It measures about 4 cm and has a diameter of about 6 mm.
The bladder base forms an angle with the posterior wall of the urethra called posterior urethrovesical angle (PUV) which normally measures 100°. The urethra runs downwards and forwards in close proximity of the anterior vaginal wall. About 1 cm from the lower end, it pierces the triangular ligament. It ultimately opens into the vestibule about 2.5 cm below the clitoris.
Relations
Posteriorly: It is related to the anterior vaginal wall to which it is loosely separated in the upper two-third but firmly adherent in the lower-third.
Anteriorly: It is related to the posterior aspect of symphysis pubis. The upper two-third is separated by loose areolar tissue; the lower one-third is attached on each side of the pubic rami by fibrous tissue called—pubourethral ligament.
Laterally:
- As it passes through the triangular ligament, it is surrounded by compressor urethra.
- Whether the medial fibers of puborectalis get attached to the urethra while passing by its sides to get attached to lateral vaginal walls is debatable.
- Bulbocavernosus and vestibular bulb.
Glands: Numerous tubular glands called paraurethral glands open into the lumen through ducts. Of these, two are longer and called Skene's ducts which open either on the posterior wall just inside the external meatus or into the vestibule. Skene's glands are homologous to the prostate in the male.
Sphincters—the following are the sphincters:
- At the urethrovesical junction, there is intricate decussation of the involuntary muscles. This has the effect of forming anterior and posterior slings which function as an involuntary internal sphincter. This is the lissosphincter. When the detrusor muscle actively contracts, the slings relax → funneling of the bladder neck → urine flows into the urethra (Fig. 1.17).11

- The wall of the urethra is composed of involuntary muscles and the fibers are arranged in the form of crossed spirals. The fibers are continuous with those of the bladder detrusor. The tone and elasticity of these muscles keep it close except during micturition.
- Sphincter urethra in the urogenital diaphragm. This sphincter allows the voluntary arrest of urine flow.
- Although debatable, puborectalis part of levator ani which surrounds the lower-third of the urethra acts as an external sphincter.
- Superficial perineal muscles, bulbocavernosus and ischiocavernosus form an accessory external sphincter.
Structures: Mucous membrane is lined by transitional epithelium except at the external urethral meatus where it becomes stratified squamous. Submucous coat is vascular. Muscle coat is composed of involuntary muscles and the fibers are arranged in the form of crossed spirals.
Blood Supply
Arterial supply: Proximal part is supplied by the inferior vesical branch and the distal part by a branch of internal pudendal artery.
The veins drain into vesical plexus and into internal pudendal veins.
Lymphatics
P. 24.
Nerves
The urethra is supplied by the pudendal nerve.
Development
The urethra is developed from the vesicourethral portion of the cloaca.
OTHER INTERNAL ORGANS
URINARY BLADDER
The bladder is a hollow muscular organ with considerable power of distension. Its capacity is about 450 mL (15 oz) but can retain as much as 3–4 liters of urine. When distended, it is ovoid in shape. It has got: (a) An apex; (b) Superior surface; (c) Base; (d) Two inferolateral surfaces; (e) Neck, which is continuous with the urethra. The base and the neck remain fixed even when the bladder is distended.
Relations: The superior surface is related with the peritoneum of the uterovesical pouch (Fig. 1.5). The base is related with the supravaginal cervix and the anterior fornix. The ureters, after crossing the pelvic floor at the sides of the cervix, enter the bladder on its lateral angles. In the interior of bladder, the triangular area marked by three openings—two ureteric and one urethral, is called the trigone. The inferolateral surfaces are related with the space of Retzius. The neck rests on the superior layer of the urogenital diaphragm.
Structures—from outside inwards:
- Outer visceral layer of the pelvic fascia.
- Muscle layer composed of muscles running in various directions. Near the internal urethral opening, the circular muscle fibers provide involuntary sphincter.
- Mucous coat is lined by transitional epithelium with no gland. There is no submucous coat.
Blood supply: The arterial supply is through superior and inferior vesical arteries. The veins drain into vesical and vaginal plexus and thence to internal iliac veins.
Lymphatics: Lymphatics drain into external and internal iliac lymph nodes.
Nerve supply: The sympathetic supply is from the pelvic plexus and the parasympathetic via the pelvic plexus from the nervi erigentes (S2,3,4). The parasympathetic produces contraction of the detrusor muscles and relaxation of the internal sphincter (nerve of evacuation). Sympathetic conveys afferent painful stimuli of overdistension.
Development: The urinary bladder is developed from the upper part of the urogenital sinus.
PELVIC URETER
The pelvic ureter extends from its crossing over the pelvic brim up to its opening into the bladder. It measures about 13 cm in length and has a diameter of 5 mm.
Course and relations: The ureter enters the pelvis in front of the bifurcation of the common iliac artery over the sacroiliac joint behind the root of the mesentery on the right side and the apex of the mesosigmoid on the left side. As it courses downwards in contact with the peritoneum, it lies anterior to the internal iliac artery and behind the ovary and forms the posterior boundary of ovarian fossa (Fig. 1.15). On reaching the ischial spine, it lies over the pelvic floor and as it courses forwards and medially on the base of the broad ligament, it is crossed by the uterine artery anteriorly (Fig. 1.11). Soon, it enters into the 12ureteric tunnel and lies close to the supravaginal part of the cervix, about 1.5 cm lateral to it. After traversing a short distance on the anterior fornix of the vagina, it courses into the wall of the bladder obliquely for about 2 cm by piercing the lateral angle before it opens into the base of the trigone. In the pelvic portion, the ureter is comparatively constricted:
- Where it crosses the pelvic brim.
- Where crossed by the uterine artery.
- In the intravesical part.
Structures: From outside inwards—(a) Fibers derived from the visceral layer of the pelvic fascia; (b) Muscle coat consisting of three layers—outer and inner longitudinal and intermediate circular; (c) Mucous layer lined by transitional epithelium.
Blood supply: The ureter has got segmental supply from nearly all the visceral branches of the anterior division of the internal iliac artery. The venous drainage corresponds to the arteries (uterine, vaginal, vesical, middle rectal, and superior gluteal).
Lymphatics: The lymphatics from the lower part drain into the external and internal iliac lymph nodes and the upper part into the lumbar lymph nodes.
Nerve supply: Sympathetic supply is from the hypogastric and pelvic plexus; parasympathetic from the sacral plexus.
Development: The ureter is developed as an ureteric bud from the caudal end of the mesonephric duct.
RECTUM
The rectum commences at the level of the third piece of the sacrum in continuation of pelvic colon and ends in anal canal. It measures 12–15 cm. The rectum follows the curve of the sacrum. It curves twice to the left and once to the right before it passes down to continue as anal canal.
Peritoneal coverings: Rectum is covered anteriorly and laterally in its upper-third, only anteriorly in the middle-third. Whole of the posterior surface and the entire lower-third remain uncovered.
Relations
Anteriorly
- The part of the rectum covered by peritoneum is related to the posterior wall of the pouch of Douglas.
- The ampulla is related to the posterior vaginal wall separated by rectovaginal septum.
- The lower part is related to the perineal body.
Posteriorly: Rectum is related to the sacrum and coccyx from which intervened by loose areolar tissue, sacral nerve trunks, and middle sacral vessels.
Laterally: Rectum is related to uterosacral ligament, pelvic plexus of nerves, and ureter. Near the anorectal junction, it is related to puborectalis part of levator ani. Below the muscle, it is related to ischiorectal fossa.
Structures
Rectum is surrounded by rectal fascia. Muscle coat consists of outer longitudinal and inner circular fibers. Submucous layer is loose and contains venous plexuses. Mucous membrane is lined by columnar epithelium.
ANAL CANAL
The anal canal measures about 2.5 cm. It is directed backwards almost at right angles to the ampulla and at the site of insertion of puborectalis part of levator ani. It ends at the anal orifice. At the junction of the upper two-third and lower one-third is the white line (Hilton's line).
Relations
Anteriorly: It is related to perineal body and posteriorly to the anococcygeal body.
Anal Sphincters
The anal canal has got two sphincters:
- Involuntary internal sphincter is formed by thickening of circular layer of the upper two-third of the anal canal.
- Voluntary sphincter ani externus which surrounds the entire length of the canal, consists of three parts:
- Subcutaneous part—it is attached to the skin.
- Superficial part—it starts from the perineal body and is inserted posteriorly to the tip of the coccyx.
- Deep part—it is separated from the sphincter ani internus by levator ani (Fig. 1.18).
Lining Epithelium
The upper two-third is lined by columnar epithelium but the lower-third with stratified squamous epithelium.
Blood Supply of Rectum and Anal Canal
Arterial supply is from:
- Superior rectal—branch of inferior mesenteric artery.
- Middle rectal—branch of internal iliac artery.
- Inferior rectal—branch of the internal iliac artery.
Venous drainage: The rectum and upper-third of the anal canal drain via superior rectal veins to portal circulation. The lower-third of the anal canal drains on both sides into inferior rectal veins (systemic system).13

Lymphatics of Rectum and Anal Canal
The lymphatics from the rectum and upper-third of the anal canal drain into internal iliac and preaortic nodes, while the lower-third of the anal canal drains into the superficial inguinal nodes.
Nerve Supply of Rectum and Anal Canal
The rectum and the upper two-third of the anal canal are supplied by autonomic through pelvic plexuses. The lower-third of the anal canal is supplied by inferior hemorrhoidal nerve.
Development of Rectum and Anal Canal
The rectum and the upper two-third of the anal canal are developed from the dorsal part of cloaca (endoderm). The lower one-third of the anal canal is developed from the anal pit (ectoderm).
PELVIC MUSCLES
The most important muscle supporting the pelvic organs is the levator ani which forms the pelvic floor. The small muscles of the perineum also have got some contribution in the support.
PELVIC FLOOR (SYN: PELVIC DIAPHRAGM)
Pelvic floor is a muscular partition which separates the pelvic cavity from the anatomical perineum. It consists of three sets of muscles on either side—pubococcygeus, iliococcygeus, and ischiococcygeus. These are collectively called levator ani. Its upper surface is concave and slopes downwards, backwards, and medially and is covered by parietal layer of pelvic fascia. The inferior surface is convex and is covered by anal fascia. The muscle with the covering fascia is called the pelvic diaphragm. Levator ani is a strong and fatigue resistant striated muscle. It is slug like a hammock around the midline pelvic effluents—urethra, vagina and anal canal (Figs. 1.19 and 1.20).
Origin
Each levator ani arises from the back of the pubic rami, from the condensed fascia covering the obturator internus (white line) and from the inner surface of the ischial spine (Fig. 1.20).


Insertion
The pubococcygeus—the fibers pass backwards and medially and are inserted as follows: (a) The posterior fibers are inserted into the anococcygeal raphe and tip of the coccyx; (b) Puborectalis—these fibers wind round the anorectal junction and are continuous with the similar fibers of the opposite side forming a ‘U’ shaped loop known as puborectal sling; (c) Puboanalis—these fibers run between the sphincter and externus and internus and are inserted in the wall of the anal canal along the longitudinal fibers; (d) Pubovaginalis—these anterior fibers pass by the side of vagina and are inserted into the perineal body (Fig. 1.19).
Coccygeus (ischiococcygeus) is triangular in shape. It arises from the apex of the ischial spine and the sacrospinous ligament and is inserted by its base into the sides of the upper two pieces of the coccyx and the last piece of sacrum (Fig. 1.19).
Anococcygeal raphe also known as levator plate, is a layered musculofibrous tissue. It extends from the anorectal junction to the tip of the coccyx. It com-prises from above downwards: (a) Presacral fascia; (b) Tendinous plate of pubococcygeus; (c) Muscular raphe of iliococcygeus; (d) Superficial fibers of sphincter ani externus muscles (Fig. 1.19).
Gaps: There are two gaps in the midline—(1) The anterior one is called hiatus urogenitalis which is bridged by the muscles and fascia of urogenital triangle and pierced by the urethra and vagina; (2) The posterior one is called hiatus rectalis, transmitting the rectum.
Structure in Relation to Pelvic Floor
The superior surface is related with the following:
- Pelvic organs from anterior to posterior are bladder, vagina and rectum.
- Pelvic cellular tissues between the pelvic peritoneum and upper surface of the levator ani which fill all the available spaces.
- Ureter lies on the floor in relation to the lateral vaginal fornix. The uterine artery lies above and the vaginal artery lies below it.
- Pelvic nerves.
The inferior surface is related to the anatomical perineum.
Nerve Supply
The muscle is supplied by the 3rd and 4th sacral nerve, inferior rectal nerve and a perineal branch of pudendal nerve (S2,3,4).
Functions
- To support the pelvic organs (Table 1.1)—the pubovaginalis which forms a ‘U’ shaped sling, supports the vagina which in turn supports the other pelvic organs—bladder and uterus. Weakness or tear of this sling during parturition is responsible for prolapse of the organs concerned.
- Counteracts the downward thrust of increased intra-abdominal pressure and guards the hiatus urogenitalis.
- Facilitates anterior internal rotation of the presenting part when it presses on the (puborectal sling) pelvic floor.
- Puborectalis plays an ancillary role to the action of the external anal sphincter.
- Ischiococcygeus helps to stabilize the sacroiliac and sacrococcygeal joints.
- To steady the perineal body.
Pelvic Floor During Pregnancy and Parturition
Due to water retention, it swells up and sags down. In the second stage, the pubovaginalis and puborectalis relax and the levator ani is drawn up over the advancing presenting part in the second stage. Failure of the levator ani to relax at the crucial moment may lead to extensive damage of the pelvic structures. The effect of such a displacement is to elongate the birth canal, which is composed solely of soft parts below the bony outlet. The soft canal has got deep lateral and posterior walls and its axis is in continuation with the axis of the bony pelvis.
PERINEUM
ANATOMICAL PERINEUM
Anatomically, the perineum is bounded above by the inferior surface of the pelvic floor, below by the skin between the buttocks and thighs. Laterally, it is bounded by the ischiopubic rami, ischial tuberosities and sacrotuberous ligaments and posteriorly, by the coccyx. The diamond-shaped space of the bony pelvic outlet is divided into two triangular spaces with the common base formed by the free border of the urogenital diaphragm. The anterior triangle is called the urogenital triangle which fills up the gap of the hiatus urogenitalis and is important from the obstetric point of view. The posterior one is called the anal triangle.
Urogenital Triangle
It is pierced by the terminal part of the vagina and the urethra. The small perineal muscles are situated in two compartments formed by the ill-defined fascia. The compartments are superficial and deep perineal pouch. The superficial pouch is formed by the deep layer of the superficial perineal fascia (Colles fascia) and inferior layer of the urogenital diaphragm (perineal membrane). The contents are (Figs. 1.3 and 1.21) superficial transverse perinei (paired), bulbocavernosus covering the bulb of the vestibule, ischiocavernosus (paired) covering the crura of the clitoris and the Bartholin's gland (paired). The deep perineal pouch is formed by the inferior and superior layer of the urogenital diaphragm—together called urogenital diaphragm or triangular ligament. Between the layers, there is a potential space of about 1.25 cm. The contents are the following muscles—deep transverse perinei (paired) and sphincter urethrae membranacea. Both the pouches contain vessels and nerves (Fig. 1.21).
Anal Triangle
The triangle has got no obstetric importance. It contains the terminal part of the anal canal with sphincter ani externus, anococcygeal body, ischiorectal fossa, blood vessels, nerves, and lymphatics.

Fig. 1.21: Schematic diagram showing pelvic muscles, fascia and cellular tissue as seen from the front.
OBSTETRICAL PERINEUM (SYN: PERINEAL BODY, CENTRAL POINT OF PERINEUM)
The pyramidal-shaped tissue where the pelvic floor and the perineal muscles and fascia meet in between the vaginal and the anal canal is called the obstetrical perineum. It measures about 4 cm × 4 cm (1½”) with the base covered by the perineal skin and the apex is pointed and is continuous with the rectovaginal septum.
The Musculofascial Structures Involved
- Fascia: (a) Two layers of superficial perineal fascia—superficial fatty layer and deeper layer called Colles fascia; (b) Inferior and superior layers of urogenital diaphragm, together called triangular ligament.
- Muscles: (a) Superficial and deep transverse perinei (paired); (b) Bulbospongiosus; (c) Levator ani—pubococcygeus part (paired) situated at the junction of the upper two-third and lower one-third of the vagina; (d) Sphincter ani externus (few fibers).
Importance
- It helps to support the levator ani which is placed above it.
- By supporting the posterior vaginal wall, it indirectly supports the anterior vaginal wall, bladder and the uterus.
- It is vulnerable to injury during childbirth.
- Deliberate cutting of the structures during delivery is called episiotomy.
PELVIC PERITONEUM
Traced anteriorly, the peritoneum covering the superior surface of the bladder reflects over the anterior surface of the uterus at the level of the internal os. The pouch, so formed, is called uterovesical pouch. The peritoneum, thereafter, is firmly attached to the anterior and posterior walls of the uterus and upper one-third of the posterior vaginal wall where from it is reflected over the rectum. The pouch, so formed, is called pouch of Douglas (Fig. 1.6).
Pouch of Douglas
This is a narrow peritoneal cul-de-sac in the pelvis situated in the rectouterine space. It is continuous with the pararectal fossa of either side.
Anteriorly, it is bounded by the peritoneal covering of the cervix, posterior vaginal fornix and upper-third of the posterior vaginal wall.
Posteriorly, it is bounded by the peritoneal covering on the anterior surface of the rectum.
Laterally, it is limited by the uterosacral folds of peritoneum covering the uterosacral ligaments.
The floor is formed by the reflection of the anterior peritoneum onto the anterior surface of the rectum. It is about 6–7 cm above the anal orifice. Below the floor, there is a thin fibrous tissue septum (rectovaginal).
Contents: It may remain empty but may contain coils of intestine or omentum.
Surgical Importance
- As it is the most dependent part of the peritoneal cavity, intraperitoneal blood or pus usually settles down to the pouch to produce either pelvic hematocele or pelvic abscess.
- Herniation of the pouch through the posterior fornix may occur producing the clinical entity of enterocele.
- Vaginal ligation is done through opening the pouch.
- Culdoscopy, culdocentesis or at time pneumoperito-neum may be done through the pouch.
- Nodules deposited in the pouch can help in the clinical diagnosis of pelvic malignancy, endometriosis or genital tuberculosis.
BROAD LIGAMENT
The double fold of peritoneum which extends from the lateral border of the uterus to the lateral pelvic wall of pelvis is called broad ligament. These are two, one on each side. These, truly are not ligaments (Fig. 1.13).
Each broad ligament consists of two layers, anterior and posterior. The layers are continuous at its upper free border embracing the fallopian tube. The lower part of the broad ligament is wider from before backwards and the layers are reflected above the pelvic diaphragm. The anterior leaf is reflected forwards at the level of the internal os as uterovesical pouch. The posterior leaf descends a little down to cover the upper-third of the posterior vaginal wall to form the posterior layer of the pouch of Douglas.
Parts of Broad Ligament
Infundibulopelvic ligament (Syn: Suspensory ligament of the ovary): It includes the portion of the broad ligament which extends from the infundibulum of the fallopian tube to the lateral pelvic wall. It contains ovarian vessels and nerves and lymphatics from the ovary, fallopian tube, and body of the uterus.
Mesovarium: The ovary is attached to the posterior layer of the broad ligament by a fold of peritoneum called mesovarium (ovarian mesentery). Through this fold, ovarian vessels, nerves, and lymphatics enter and leave the hilum. The ovary is not enclosed within the broad ligament (Fig. 1.13).
Mesosalpinx: The part of the broad ligament between the fallopian tube and the level of attachment of the ovary is the mesosalpinx. It contains utero-ovarian anastomotic vessels and vestigial remnants (Fig. 1.13).
Mesometrium: The part of the broad ligament below the mesosalpinx is called mesometrium. It is the longest portion which is related with the lateral border of the uterus.
Contents
Each broad ligament contains:
- Fallopian tube.
- Uterine and ovarian arteries with their branches, including the anastomotic branches between them and corresponding veins.
- Proximal part of the round ligament which raises a peritoneal fold on the anterior leaf.
- Ovarian ligament which raises a peritoneal fold on the posterior leaf.
- Parametrium containing loose areolar tissue and fat. The terminal part of the ureter, uterine artery, paracervical nerve, and lymphatic plexus are lying at the base of the broad ligament.
- Vestigial structures, such as duct of Gartner, epoophoron, and paroophoron.
Development
The broad transverse fold which is established as the two Müllerian ducts approach each other is developed into broad ligament.
Function
Along with the loose areolar tissue (packing material), it has got steadying effect to maintain the uterus in position.
PELVIC FASCIA AND CELLULAR TISSUE
PELVIC FASCIA
For descriptive purpose, the pelvic fascia is grouped under the heading that covers the pelvic wall, the pelvic floor, and the pelvic viscera.
Fascia on the Pelvic Wall
The fascia is very tough and membranous. It covers the obturator internus and pyriformis and gets attached to the margins of the bone. The pelvic nerves lie external to the fascia but the vessels lie internal to it.
Fascia on the Pelvic Floor
The fascia is not tough but loose. The superior and the inferior surfaces are covered by the parietal layer of the pelvic fascia which runs down from the white line to merge with the visceral layer of the pelvic fascia covering the anal canal (Fig. 1.21).
Fascia Covering the Pelvic Viscera
The fascia is not condensed and often contains loose areolar tissue to allow distension of the organs.
PELVIC CELLULAR TISSUE
The cellular tissue lies between the pelvic peritoneum and the pelvic floor, and fills up all the available empty spaces. It contains fatty and connective tissues and unstriped muscle fibers. Collectively, it is known as endopelvic fascia. Its distribution round the vaginal vault, supravaginal part of the cervix and into the layers of the broad ligament is called parametrium. Condensation occurs especially near the cervicovaginal junction to form ligaments, which extend from the viscera to the pelvic walls on either side. The deep endopelvic connective tissue condenses to form: (a) Uterosacral ligaments; (b) Cardinal ligaments; (c) Pubocervical ligament; (d) Rectovaginal septum; (e) Pubovesical fascia.
MACKENRODT'S LIGAMENTS (SYN: CARDINAL LIGAMENT, TRANSVERSE CERVICAL)
Origin: Condensation of parietal fascia covering the obturator internus.
Insertion: Lateral supravaginal cervix and upper part of lateral vaginal wall in a fan-shaped manner. This insertion is continuous with the endopelvic and pericervical fascial ring.
Content: Uterosacral plexus of autonomic nerves, uterine artery, and vein, smooth muscle fiber. Distal part of ureter passes under the uterine artery within the upper part of the cardinal ligament. It is situated inferior to the uterosacral ligament with which it is blended (Fig. 1.22).

18Function: (a) Lateral stabilization to the cervix at the level of ischial spine; (b) Primary vascular conduits of the uterus and vagina.
UTEROSACRAL LIGAMENTS
Origin: Periosteum of sacral vertebra 2, 3, and 4.
Insertion: Posterolateral surface of the cervix at the level of internal os. Here it blends with the endopelvic fascial ring. These are formed by condensation of peritoneum.
Content: Uterosacral plexus of autonomic nerves. Smooth muscle and minimal vessels.
Function: These are the primary proximal suspensory ligaments of the uterovaginal complex. They hold the cervix posteriorly at the level of the ischial spines. Uterus is thus maintained anteflexed and the vagina is suspended over the levator plate.
PUBOCERVICAL FASCIA (BLADDER PILLAR)
Origin: Back of the pubic bone and the arcus tendineus fascia laterally.
Insertion: Anterolateral supravaginal cervix and blends with the pericervical ring of endopelvic fascia and the cardinal ligaments.
Content: Artery and veins of the bladder pillar.
Function: These ligaments are poorly developed. They serve mainly as vascular conduit and provide less cervical stabilization force.
Vesicovaginal septum: It is a fibroelastic connective tissue with some smooth muscle fibers.
Extension: Laterally, it extends from pubic tubercles, pubic arch. Arcus tendineus fascia (white line) and centrally to the pubocervical ring, blending with the pubocervical and cardinal ligaments, and pelvic visceral fascia.
Function: It supports the bladder and the anterior vaginal wall.
Rectovaginal septum (RVS) (Fascia of Denonvilliers’): It is also a fibroelastic connective tissue with few smooth muscle fibers.
Extension: It is an extension of endopelvic fascia. It extends between the posterior vaginal wall and anterior wall of the rectum. This fibroelastic connective tissue fuses below with the perineal body, centrally with the pericervical ring, laterally to the arcus tendineus fascia, Mackenrodt's ligament and posteriorly with the uterosacral ligaments.
Function: It supports the posterior vaginal wall, stabilizes the rectum and the perineum.
Pericervical ring (Fig. 1.22): It is a circular band of fibromuscular connective tissue that encircles the supravaginal part of the cervix.
Extension: Anteriorly, it lies between the base of the bladder and the anterior cervix. It is continuous with the pubocervical ligaments.
Laterally: It is continuous with the Mackenrodt's ligaments.
Posteriorly: It is located between the posterior surface of the cervix and the rectum behind. It extends posteriorly as the uterosacral ligaments.
Function: It stabilizes the cervix at the level of ischial spines.
ROUND LIGAMENTS
These are paired, one on each side. Each measures about 10–12 cm. It is attached at the cornu of the uterus below and in front of the fallopian tube. It courses beneath the anterior leaf of the broad ligament to reach the internal abdominal ring (Figs 1.11 and 1.15). After traversing through the inguinal canal, it fuses with the subcutaneous tissue of the anterior third of the labium majus. During its course, it runs anterior to obturator artery and lateral to the inferior epigastric artery (Fig. 1.15). It contains plain muscles and connective tissue. It is hypertrophied during pregnancy and in association with fibroid. Near the uterus, it is flat but more distally, it becomes round. It corresponds developmentally to the gubernaculum testis and is morphologically continuous with the ovarian ligament. The blood supply is from the utero-ovarian anastomotic vessels. The lymphatics from the body of the uterus pass along it to reach the inguinal group of nodes. While it is not related to maintain the uterus in anteverted position, but its shortening by operation is utilized to make the uterus anteverted.
Embryologically, it corresponds with gubernaculum testis. In the fetus, there is a tubular process of peritoneum continuing with the round ligament into the inguinal region. This process is called canal of Nuck. It is analogous to the processus vaginalis which precedes to descent of the testis.
OVARIAN LIGAMENTS
These are paired, one on each side. Each one is a fibromuscular cord-like structure which attaches to the inner pole of the ovary and to the cornu of the uterus posteriorly below the level of the attachment of the fallopian tube (Fig. 1.13). It lies beneath the posterior leaf of the broad ligament and measures about 2.5 cm in length. Morphologically, it is continuous with the round ligament and together are homologous to the gubernaculum testis.19