

INTRODUCTION
Approximately 15% of couples are unable to conceive after one year of unprotected intercourse. A male factor is solely responsible in about 20% of infertile couples and contributory in another 30-40%1 and another study by Hull et al, 1985;2 1992,2 suggested spermatozoan defects accounting for some 30-50% of cases of sub-fertility. Although the semen analysis is not a test of fertility, it is the most important single indicator of the functional status in the male reproductive tract. Clinical studies of infertile patients have established “limits of adequacy” below which the chance of initiating a pregnancy becomes more difficult. A minimum of two evaluations is recommended to establish a profile of the seminal parameters.
An initial screening evaluation of the male partner of an infertile couple should be done if pregnancy has not occurred within one year of unprotected intercourse. An earlier evaluation may be warranted if a known male or female infertility risk factor exists or if a man questions his fertility potential. The initial evaluation for male factor infertility should include a reproductive history and two properly performed semen analyses. A full evaluation by a urologist/andrologist or other specialist in male reproduction should be done if the initial screening evaluation demonstrates an abnormal male reproductive history or an abnormal semen analysis. Further evaluation of the male partner should also be considered in couples with unexplained infertility and in couples in whom there is a treated female factor and persistent infertility.
SEMEN ANALYSIS
Semen analysis is the cornerstone of the laboratory evaluation of the infertile male and helps to define the severity of the male factor. The first person to suggest that semen4 analysis should be a routine investigation in the evaluation of every case of infertility was Edward Martin5 (1902; cited by Jequier, 1991). Martin also demonstrated that there were two major causes of azoospermia and he was also the first to recognize the polymorphism of human sperm. John MacLeod then elevated semen analysis from being a simple observation into a science. He recognized that not only sperm numbers but sperm motility and morphology were also important in the evaluation of the potential fertility of semen.6 He even tried to associate certain sperm shapes with specific clinical entities such as Varicocele.7 However, many clinicians and laboratory personnel did not follow MacLeod's lead in relation to semen analysis. In or around 1980, it became clear, that many laboratories worldwide were not even attempting to examine a number of variables within a semen sample that were important in the determination of fertility. Often only an estimation of the sperm concentration was being performed and no assessment of either motility or morphology was made by a number of pathology laboratories. Thus what information that could be obtained from the examination of semen was not being sought.8
By the early 1980s, however, Mortimer and colleagues were anxious to further advance the understanding of the inter-relationships between the different variables in a semen analysis9 and also introduced the concept of quality assurance in relation to the analysis of semen.10 It is now very clear that careful training in semen analysis, such as that set up by the ESHRE Andrology Special Interest Group that includes both theoretical as well as practical training in semen analysis, is very effective in raising the skills of laboratory personnel in relation to semen analysis.11
However, it should be understood that semen analysis is a guide to fertility and not an absolute proof of fertility of an individual. Over time it has become clear that the relationship between infertility and sperm numbers, sperm movement and sperm morphology is not a simple one. It has been known for a long time that reproductive pathology in the female partner reduces the potential fertility of a male with a ‘normal’ sperm count12 while a high sperm count such as that achieved using donated sperm can overcome female problems that could otherwise result in childlessness.13 Thus the male-female interaction in infertility is immensely important to the outcome in relation to pregnancy, and this inter-relationship cannot in any way be incorporated into a semen analysis.
The literature in relation to the fate of the sperm once they enter the female genital tract in the human is very sparse. However, it is clear that, of the total number of sperm that enter this tract in a conception cycle, all but one are lost. Many of the sperm also drain out of the vagina after coitus in the phenomenon also known as ‘flowback’. What percentage of the ejaculate enters the cervical mucus is unclear but it is probably small. Of those sperm entering the cervical mucus, a proportion may become eliminated by their passage into the folds of the cervical epithelium and by their entry into the cervical glands.14 Many sperm also loose or change their motility on entering the cervical mucus.155
The numbers of sperm that traverse the uterine cavity in the human and reach the utero-tubal junctions in the human is unknown but probably only a few thousand sperm enter each Fallopian tube.16 Those sperm that do succeed in entering the Fallopian tubes will therefore only make up a very small percentage of the total numbers seen in the whole ejaculate.
Due to the relatively vast surface area of the heaped-up epithelium of the Fallopian tubes (certainly vast in relation to the size of a spermatozoon), only a relatively small number of sperm will be able to access the oocyte. Not only must the sperm traverse the corona but they must also be able to exhibit hyperactivated movement and must not have undergone the acrosome reaction until they are close to the zona pellucida. It is thus also possible that human fertilization may depend frequently upon a sperm oocyte ratio that may be as low 1:1.
Methods of semen analysis are discussed in many textbooks, and detailed laboratory protocols have been published by the World Health Organization (WHO).17–20 In view of the need to standardize laboratory techniques and determine normal semen parameters, the World Heath Organization (WHO) published its Laboratory Manual for Examination of Human Semen and Semen-Cervical Mucus Interaction, in 1980.17 Subsequently, revisions were published in 1987,18 199219 and 1999.20
The WHO criteria of 1987 and 199218,19 which classify more sperm in the normal category, are also widely used in the routine semen evaluation, however there is a need to standardize the reports to the latest WHO criteria 1999.20 True reference ranges have not been established for semen parameters. The reference values in Table 1.1 are based on the clinical literature. Values that fall outside these ranges suggest a male infertility factor and indicate the need for additional clinical and/or laboratory evaluation of the patient.21 It must be emphasized that the reference values for semen parameters are not the same as the components of a full evaluation for male infertility.22
SEMINAL FLUID ANALYSIS—METHODOLOGY
The use of standardized laboratory protocols, such as those described by the World Health Organization is clearly desirable, as “ a major reason why the basic assessments of semen have variable predictive value is due to a high degree of error in the techniques used to assess the samples.” To ensure accurate results, the laboratory should have a quality control program for semen analysis, which conforms to the standards outlined in the Clinical Laboratory Improvement Amendments (CLIA). Information on these standards, which include proficiency testing, can be found at the CLIA web site.23 The availability of semen renders possible direct examination of male germ cells, giving precious data that are not accessible for female germ cells.6
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Semen analysis includes the examination of:
- Spermatozoa
- Other cells present in semen
- Seminal fluid
Altogether these data give indications on the testicular function and of the integrity of the male genital tract which may facilitate treatment plans.7
Type of Assays
1. Descriptive assay: | Seminogram |
2. Functional assays: | Penetration of cervical mucus (postcoital test, in vitro penetration assay) Binding of sperm to the zona pellucida Fusion of sperm with zona-free hamster oocyte Hypo-osmotic swelling of the flagella |
3. Immunological assay: | Mixed agglutination test immunobead test Sperm immobilization in cervical mucus |
Guidelines and Parameters
The guidelines and parameters to look for in a semen analysis are listed below.20
Safe Handling of Biological Specimens
It is important good laboratory practice is followed and a sterile jar collection is observed when collecting semen samples as they may contain harmful viruses or the samples may get contaminated.
Sample Collection and Delivery
Physicians should provide patients with standard instructions for semen collection. These instructions should include a defined period of abstinence of two to three days. Semen can be collected by masturbation or by intercourse using special semen collection condoms that do not contain substances detrimental to sperm. The specimen may be collected at home or at the laboratory. The specimen should be kept at room or body temperature during transport and examined within one hour of collection.
Collection Method and Abstinence Periods
The ejaculate should be collected by masturbation into the sterile, non-toxic, wide necked collection jar provided and not by withdrawal or by using a contraceptive condom. It is important to note that contamination of the semen sample with either saliva, soap or water may adversely affect sperm quality. In exceptional circumstances only, should a couple be provided with a special non-toxic silastic condom. The sample should be collected after a minimum of 48 hours but no longer than seven days of sexual abstinence.
Table 1.2 shows that the semen volume and sperm concentration increased according to how the number of days of sexual abstinence. However, in patients with five or more days of sexual abstinence, a reduction in progressive motility was found. The sperm morphology did not vary with length of sexual abstinence.8
Initial Evaluation of Sample
Note the following basic information:
- Duration of abstinence
- Sampling (complete or spillage)
- Time of sample collection and method of sampling (masturbatory or coital)
- Appearance (abnormal smell, color, blood)
Semen is normally translucent or whitish-gray opalescent in color.
Viscosity of the ejaculate: After ejaculation the seminal secretions form a coagulum which gradually liquefies. Semen is normally produced as a coagulum. The specimen usually liquefies within 30 minutes. The failure to liquefy within one hour is abnormal. In most cases, the semen sample should become fully liquefied within 60 minutes of production and if liquefaction time is above 60 minutes, the sample may be treated with bromelin to facilitate liquefaction.
Non-liquefaction and excessive viscosity are two separate conditions. Viscosity is measured after complete liquefaction has occurred. Viscosity is considered “normal” if the liquefied specimen can be poured from a graduated beaker drop by drop with no attaching agglutinum between drops. The viscosity of a semen sample is a reflection of the mucus content. With excessively viscous samples, thorough mixing can be difficult and accurate estimation of sperm concentration and motility may be impossible. Seminin is the agent primarily responsible for liquefaction of the seminal coagulum in men and spermatozoa do not influence liquefaction. The role of hyper (excessive) viscosity is being studied, but it seems possible that this condition may interfere with the ability of sperm to travel from the site of deposition into the cervix or uterus.9
Volume of the Ejaculate
Measured by weight, normal volume is 1.5 to 6 ml. Semen volume per se, however, affects fertility only when it falls below 1.5 cc, due to the inadequate buffering of vaginal acidity or when the volume is greater than 6 cc. Low volumes may be associated with incomplete collection, retrograde ejaculation, ejaculatory duct obstruction, or androgen deficiency.
pH
Ideally this should be performed within 60 minutes of ejaculation and is measured with pH paper. The normal pH of semen is slightly alkaline (7.2-8.0) but increases with time. Prostatic secretions are acidic while the secretions of the seminal vesicles are alkaline. Therefore, alterations in pH may reflect a dysfunction of one or both of these accessory glands. The pH of semen has not been generally found to have a major influence on a man's fertility potential.
Fructose Assessment
If no spermatozoa are observed, a qualitative test for fructose should be performed. A low ejaculate volume and lack of fructose, along with failure of the semen to coagulate, suggest congenital absence of the vas deferens and seminal vesicles or obstruction of the ejaculatory ducts. Fructose is androgen-dependent and is produced in the seminal vesicles and very useful to differentiate ejaculatory duct obstructions or lower genital tract pathology.
Semen Analysis Sample (Wet) Preparation—Concentration
The improved Neubauer hemocytometer (Fig. 1.1) should be used for the estimation of spermatozoal concentration with a phase contrast microscope.


The semen should be diluted in a suitable buffer and the dilution factor adjusted according to the “guestimate” of sperm concentration observed on the wet preparation. The sperm should then be counted - do not count headless or “pin-heads” sperm and do not count tailless heads. Sperm concentrations of less than 20 million/ml are classified as oligospermic. This figure probably derives mainly from the work of MacLeod, who found that only 5% of fertile men had sperm concentrations less than 20 million/ml.6
Azoospermia should not be diagnosed until the specimen is centrifuged at maximum speed (preferably 3000 gm) for 15 minutes, and the pellet is examined.
Motility Assessment
Spermatozoa, after passage through the epididymis, are motile cells. Sperm motility becomes critical at the time of fertilization, because it allows or at least facilitates passage of the sperm through the zona pellucida. Without technologic intervention, a non-motile or abnormally-motile sperm is not going to fertilize. Hence, assessing the fraction of a sperm population that is motile is perhaps the most widely-used measure of semen quality.
There are four classifications of motility:
- Rapid progressive motility - the sperm are moving swiftly across the field usually in a straight line
- Slow or sluggish progressive motility - the sperm may be less linear in their progression
- Non-progressive motility - sperm are also described as twitching or shaking
- Immotility—sperm do not move at all.
A progressively motile sperm swims forward in an essentially straight line, whereas a non-progressively motile sperm swims, but with an abnormal path, such as in tight circles. A sample of semen is diluted in buffered saline, and about 10 to 20 microliters of this sample is pipetted onto a clean, prewarmed microscope slide. A coverslip is lowered onto the sample, avoiding formation of air bubbles if possible, and the slide is examined using a microscope with a 20X objective. At least ten widely-spaced fields are examined to provide an estimate of the percentage of motile cells. Spurious asthenospermia because of exposure of sperm to rubber (particularly condoms), spermicides, extremes of temperature, or long delays between collection and examination should be excluded before accepting that sperm motility is poor. Low sperm motility is a frequent accompaniment of oligospermia, and there usually is a mixed picture of morphological defects. It presumably arises because of defective spermiogenesis.
A bright field microscope can be used for evaluating motility if the field diaphragm is closed to enhance contrast and ability to visualize sperm. A much better choice is a phase contrast microscope or a microscope equipped for differential interference contrast (DIC). Examine the images to appreciate the difference in these three types of microscopy—clearly, unstained sperm are difficult to observe using bright field (Fig. 1.2).11

Severe asthenospermia requires evaluation by electron microscopy.27 Specific ultrastructural defects of the axoneme are associated with zero sperm motility or extreme asthenospermia (less than 5% motile sperm) and sterility.28 Absent dynein arms, other less common axonemal defects, mitochondrial abnormalities, disorganized fibrous sheath or outer dense fibers with stumpy tails, or normal ultrastructure may be found.29 The gene defects in some of these disorders are being discovered. Standard semen analyzes of these patients usually show normal sperm concentrations and normal sperm morphology, although some have tail abnormalities at the light microscopic level—short, straight, or thick tails or mid-piece defects. Motility is graded in the following fashion.20
Poor motility could be due to many factors such as hormone deficiency, varicocele, infection, drugs such as antidepressants, antihypertensive drugs, anabolic steroids, cocaine, heavy smoking and excess alcohol. Other causes include frequent hot baths and saunas. Testicular cancer is also associated with an increased risk of impaired sperm production (it occurs in middle age men, whereby the risk is increased in men who have had a history of undescended testicles). Furthermore, antisperm antibodies may adversely affect sperm production.
Assessment of Sperm Morphology
The evaluation of sperm morphology is performed after Papanicolaou or similar staining and consists in detailed examination of 100 sperm cells as well as other cells present in the ejaculate, including leukocytes and immature sperm cells (Fig. 1.3). Although the methods for routine measurement of sperm concentration and motility have changed little during the past two decades, sperm morphology assessment has evolved considerably (Figs 1.4 and 1.5).12
The current WHO criteria for scoring sperm morphology20,24 are similar to the Kruger (Tygerberg) strict criteria (Fig. 1.6),30,31 in that relatively few sperm are classified as having normal morphology, even in semen from fertile men. Sperm morphology assessment by strict criteria is used to identify couples who have a poor chance of fertilization with standard in vitro fertilization (IVF)26 or a better chance of fertilization with ICSI.25,26 The WHO criteria of 1987 and 199218,19 which classify more sperm in the normal category, are also widely used in the routine semen evaluation.
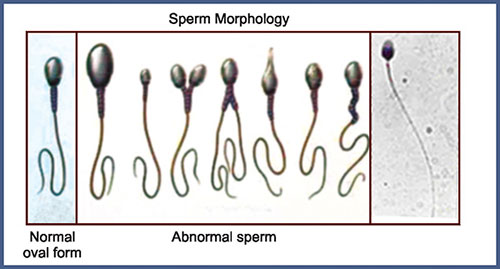
A normal spermatozoa should have a oval shaped head (4-5.5 µm long and 2.5-3.5 µm wide). The midpiece should be cylindrical (3-5 µm long and 1.0 µm wide). The tail should also be cylindrical (45-50 µm long and 0.5 µm wide) with a narrower terminal segment (4-6 µm long). There should be no head, midpiece or tail defects, and no cytoplasmic droplet more than one-third the size of a normal sperm head (Fig. 1.7).
Spermatozoa which do not fit this description should be considered ‘abnormal’, and classified according to the defects detailed below. Only recognizable sperm should be included—do not score immature germ cells as spermatozoa. All “borderline” forms should be considered abnormal.
Numerous references can be found in the literature which seek to establish the clinical relevance of abnormal sperm morphology,30,32 and it is generally accepted that a high incidence of morphologically abnormal spermatozoa in a semen sample is associated with reduced fertility. The WHO recommends an empirical reference value,20 that 30% or more of the spermatozoa in an ejaculate should be normal forms.
The rare cases of monomorphic teratozoospermia as well as severe asthenozoospermia33 can be subjected to Electron Microscopic analysis to detect specific defects at the ultrastructural level, particularly in the flagella where abnormal microtubule assembly can be found as in the immotile cilia syndrome.13

Fig. 1.4: Spermatozoa showing tail defects: (A) Short tail, (B) Coiled tail, (C) Short coiled tail, (D) Thick tail, (E) Long tail, (F) Double tail, (G) Cytoplasmic droplet present on tail, (H) Thin tail, (I) Bent tail

Fig. 1.5: Spermatozoa showing normal spermatozoa, Mid piece defect and other defects. BM—Bent mid piece defect, MD—Multiple defect, ED—Elongated head defect, ST—Short tail defect, N—Normal spermatozoa


Agglutination
The presence of agglutination or clumping of sperms should be recorded as this may indicate immunological infertility. Both autoimmunity and isoimmunity have been found responsible in 12.5% of couples of primary infertility and 10% of couples of secondary infertility. As many as, 21% of cases of unexplained infertility were attributed to presence of antibodies in sera of infertile couples.
Other Cells in Semen
The presence of other cell types in human semen other than spermatozoa are common and include leukocytes (white blood cells), epithelial cells and immature germ cells. They15 are collectively referred to as “round cells”. The number of round cells can be estimated in wet preparations using a suitable counting chamber (Fig. 1.8). To accurately diagnose leukocytospermia (which can indicate reproductive tract infection), then it is important to identify actual leukocytes using a suitable staining technique. Large numbers of round cells is not necessarily a positive diagnosis of infection.
Excessive white cells (> 1 million/cc) may indicate an infection that may contribute to subfertility and an elevated number of white blood cells in the semen has been associated with deficiencies in sperm function and motility. Under wet mount microscopy, both leukocytes and immature germ cells appear similar and are properly termed “round cells.” Many laboratories improperly report all round cells as “white blood cells.” The clinician must make sure that the two types of cells are differentiated. The distinction between spermatogenesis cells and leukocytes is not always obvious, and it is important particularly in cases of azoospermia. Indeed, in azoospermia, the presence of spermatogenesis cells indicates a testicular malfunction, while the presence of leukocytes in the absence of any spermatogenesis cells suggests that the azoospermia might be due to an obstruction problem.
Spermatogenesis cells present in semen are usually degenerating, and can sometimes be confused with leukocytes. In particular, multinucleated spermatids (immature germ cells) can be confused with polymorphonuclear leukocytes (PMN). Staining of endogenous peroxidases present in PMN can help to distinguish between these two cell types as also immunohistochemical techniques.34 Those patients with true pyospermia (greater than 1 million leukocytes per ml) should be evaluated for a genital tract infection or inflammation.

Fig. 1.8: A cluster of spermatogenic cells and leukocytes. L—Leukocyte, S—Spermatogenic cell/round cell
Large numbers of epithelial cells in semen may be an indication of infection or overactive masturbation. Similarly the presence of red blood cells (erythrocytes) may indicate a reproductive tract infection, tuberculosis or damage to a small capillary during sample production. Bacterial and protozoal infections are uncommon in human semen but their presence is indicative of possible male reproductive tract infection and should be reported to the referring doctor for further evaluation.
Assessment of Sperm Viability/Vitality
Sperm viability can be assessed by mixing fresh semen with a supravital dye such as eosin or trypan blue, or by the use of the hypo-osmotic swelling (HOS) test.20 These assays determine whether non-motile sperm are viable by identifying which sperm have intact cell membranes. As the plasma membranes of dead spermatozoa are permeable, only dead cells will stain, live cells are unstained (Fig. 1.9). Non-motile but viable sperm, as determined by the HOS test, may be used successfully for ICSI.
Clearly, a sperm which is moving however feebly, is ‘alive’. If the percentage of immotile sperm exceeds 50%, then the proportion of live spermatozoa should be determined. This is important since conditions exist (e.g. immotile cilia syndrome/Kartageners syndrome) where all the sperm may be immobile but alive, such conditions are now treatable using intracytoplasmic sperm injection (ICSI).
Table 1.3 provides a brief insight into the common seminal abnormalities.

| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Additional Tests
Post-ejaculatory Urinalysis
Low-volume or absent ejaculate suggests retrograde ejaculation lack of emission, ejaculatory duct obstruction, hypogonadism. In order to diagnose possible retrograde ejaculation, the physician should perform a post-ejaculatory urinalysis for any man whose ejaculate volume18 is less than 1.5 ml, and who has not been diagnosed with hypogonadism. It is also important to assure that improper or incomplete collection, or a very short abstinence period (less than 1 day) is not the cause of the low-volume ejaculate. The post-ejaculatory urinalysis is performed by centrifuging the specimen for 10 minutes at a minimum of 300 gm.
Biochemical Analysis
Seminal fluid parameters: Biochemical assays of markers for prostate, seminal vesicles and epididymis assess the function of these accessory glands. These markers include fructose as seminal vesicles marker, zinc or acid phosphatase as prostate marker and carnitine as epididymis marker. Zinc can be measured by colorimetric assay while fructose and carnitine are measured using enzymatic assays.
Bacteriological Analysis—Semen Cultures
Direct measurement of infectious contamination is obtained from aerobic and anaerobic cultures to rule out specific genital tract infection. In normal conditions semen is not sterile but rather colonized at low levels by a variety of microorganisms. Recent studies have shown that bacterial colonization did not have negative impact on sperm-cervical mucus interaction.
If urinalysis is abnormal or bacterial prostatitis is implicated by either the history or physical examination, appropriate cultures are indicated. The common sexually transmitted organisms such as Chlamydia trachomatis, Mycoplasma hominis and Ureaplasma urealyticum have been implicated in reproductive failure in animals and humans. On the basis of this supposition, physicians have instituted antibiotic therapy without obtaining evidence of infection in the hope of improving fertility. Currently there is no evidence for the role of asymptomatic infection due to the above organisms in male infertility. Without evidence of inflammation, there is no indication for routine culture or antibiotic treatment of infertile men.
Sperm-Cervical Mucus Interactions
Cervical mucus is the major physical barrier that sperm cells have to cross to access the female upper genital tract. Less than 1% of the sperm deposited in the vagina successfully penetrate the cervical mucus. Evaluation of sperm-cervical mucus interactions include the postcoital test, the sperm cervical mucus contact test and the in vitro sperm-cervical mucus penetration assay.
Postcoital Test
The postcoital test is the analysis of cervical mucus a few hours after intercourse. It reflects the physiologic situation in vivo and assess both the quality of cervical mucus and the19 penetration ability of sperm. Postcoital tests are scheduled just before ovulation as determined by basal body temperature, or more accurately by follicular sizing by ultrasonography. The number of motile sperm per high power microscopic field is recorded and the test is considered positive when 10 or more motile sperm are found per field according to WHO guidelines. Cervical mucus evaluation (including volume, consistensy, ferning, spinnbarkeit, cellularity and pH) is of utmost importance for the interpretation of postcoital test results with respect to sperm function. A decreased number of sperm in cervical mucus when the cervical mucus score is low reflects inadequate mucus rather than impaired sperm function. Sperms are present in cervical mucus constantly for at least 12 hours following intercourse and the timing of postcoital test (6-12 hours after intercourse) allows to test the viability of sperm in this environment.
The postcoital test has been used for several decades but is reported to be inaccurate and lacks consensus on normal values and methodology.44 Part of the problem may be due to the non-homogeneous nature of the cervical mucus that prevents quantitative determination of sperm concentration. Contemporary treatments for otherwise unexplained infertility, such as superovulation and intrauterine insemination or in vitro fertilization, effectively negate any unrecognized cervical factors. Routine postcoital testing is unnecessary. The test may be reserved for patients in whom results will influence treatment strategy.45
Sperm-Cervical Mucus Contact Test
Sperm-cervical mucus contact test consists in mixing semen and cervical mucus in vitro and measuring the appearance of immobilized “shaking” motile sperm. This test can be performed in parallel with donor semen or donor cervical mucus, and therefore allows to discriminate between a male versus female origin of the sperm immobilizing factor.
In vitro Cervical Mucus Penetration Test
The third test of sperm-cervical mucus interactions involves the penetration of cervical mucus by sperm in vitro. The mucus is placed in a capillar tube, one end of the tube is dipped in semen and penetration and motility of sperm in the mucus column is measured. It can be performed with homologous or donor cervical mucus. Using cervical mucus standardized by estrogen treatment, this test was shown to have good predictive value of fertility. Alternatively to human cervical mucus this test can be performed with commercial midcycle bovine cervical mucus or hyaluronic acid gels. The use of alternative material to human cervical mucus has practical advantages (availability, reproducibility) but may be less informative than human material, due to differences in the nature of the hydrogels. Therefore, whenever possible human cervical mucus should be used and for specific male factor detection estrogen standardized donor mucus should be preferred.20
Detection of Antisperm Antibodies
Pregnancy rates may be reduced by antisperm antibodies (ASA) in the semen.35 In the infertile population as a whole, autoimmune anti-sperm antibodies (ASABs) occur in 5-10% of individuals (Matson, 1994).36 Spermatogenesis starts at puberty, after the “education” of the immune system to recognize self antigens is finished and are therefore immunogenic. Under normal circumstances they are protected from the man's immune system by the hemato-testicular barrier that separates the inner part of seminiferous tubules from the blood. When this barrier is ruptured sperm cells induce the synthesis of anti-sperm antibodies. Antibodies adsorbed on the sperm surface can be detected by immunological assays using secondary, Ig class-directed antibodies that are coupled to beads. The percentage of sperm adhering to the beads reflects in a semi-quantitative manner the presence of anti-sperm antibodies.
The mixed antiglobulin reaction test (Mar-test) is widely used to detect anti-sperm IgG in semen. WHO consider this an adequate routine screening test since IgA antibodies almost never occur without IgG antibodies (WHO, 1992,19). Positive and dubious samples are subsequently tested for anti-sperm IgA. IgA antibodies are more significant clinically, but very rarely occur without associated IgG. Therefore the test of anti-sperm IgG antibodies in semen is sufficient for the first screening procedure. Anti-sperm IgG can be tested in serum but this is of little benefit as serum anti-sperm IgG do not correlate with anti-sperm Ig in semen and do not influence fertility prognosis.
Risk factors for ASA include ductal obstruction, prior genital infection, testicular trauma and prior vasovasostomy or vasoepididymostomy. ASA testing should be considered when there is isolated asthenospermia with normal sperm concentration, sperm agglutination or an abnormal postcoital test. Many physicians recommend ASA testing for couples with unexplained infertility. ASA found on the surface of sperm by direct testing are more significant than ASA found in the serum or seminal plasma by indirect testing. ASA testing is not needed if sperm are to be used for ICSI.
Sperm Functional Assays
Sperm functional assays have been developed in an attempt to find a good predictive test of male fertility. They include sperm cervical mucus interactions, the sperm hypo-osmotic swelling assay, hemizona assay and the hamster egg penetration assay.
Hypo-osmotic Swelling Test—HOST
It has been found that when sperm from normal fertile men are exposed to a known solution of fructose and sodium citrate, 33-80% of the spermatozoa will exhibit tail swelling.21 Sperm that are not viable or sperm with non-functioning membranes do not swell. This appears to be explained by the ability of the normal cell membrane to maintain an osmotic gradient (Fig. 1.10). Attempts have been made to correlate this finding with the fertilization potential for semen samples. Samples with greater than 62% swelling are able to fertilize ova, whereas less than 60% swelling is observed in samples of infertile semen. The biologic significance of this test is unclear and its validity to predict IVF rate is controversial, and it is equivalent to viability staining.37
Acrosomal Intactness and Seminal Hyaluronidase Activity Test
There is a highly significant correlation between seminal hyaluronidase activity and acrosomal intactness scores. This could be because; normal germinal semineferous epithelium generates abundant number of sperms with normal motility and morphology that are also having intact acrosome. Intact acrosome prevents loss of acrosomal enzymatic activity (e.g. hyaluronidase) until released after liquefaction during seminal analysis and during acrosomal reaction in female genital tract prior to fertilization. Seminal hyaluronidase activity, thus determined, is primarily dependent upon the intact status of acrosome (Fig. 1.11). As each sperm contributes to the seminal hyaluronidase activity, it is directly correlated with sperm density; but at the same time it exhibits good correlation with % motility and % normal morphology. Therefore AI score and seminal hyaluronidase activity can be considered as good indicators of sperm function.38

Fig 1.10: Hypo-osmotic swelling test—Spermatozoa showing coiled tail and non-coiled tail. CT—coiled tail, NCT—non-coiled tail

Fig 1.11: Acrosomal intactness (AI): Spermatozoa showing heads with halos and without halos. WH—with Halo, AH—absence of Halo

Fig. 1.12: Nuclear chromatin decondensation test: Spermatozoa showing decondensed heads and condensed heads. D—decondensed head, C—condensed head
Nuclear Chromatin Decondensation (NCD) Test
Heterospecific in vitro fertilization necessitates the completion of the capacitation, the acrosome reaction, and the nuclear decondensation into the ooplasm. Chromatin stability is an important determinant of semen quality, essential for spermatozoa maturation in epididymes and early embryogenesis (Fig. 1.12). Changes in the chromatin stability are essential for maturation of mammalian spermatozoa, egg fertilization and embryonic23 development. Chromatin is stabilized by the disulphide bridges (S-S) between adjacent protamines. Zinc ions and seminal plasma may play a role in the formation of S-Zn-S bridges, which additionally stabilize the chromatin structure. Reduced glutathione, heparin and albumin levels have been found in the secretions of a female reproductive tract and are physiological decondensing agents of sperm nuclei. Reduced glutathione, a disulphide bridge reducing agent, albumin and heparin which binds specifically to the sperm plasmalemma, have been shown to induce nuclear decondensation of human spermatozoa.39,40 However, the precise role of NCD test in fertility is controversial.
Sperm Mitochondrial Activity Index (SMAI) Test
It is postulated that proper mitochondrial development of late spermatids and spermatozoa was necessary for fertilization and any process which affects this development could lead to azoospermia. This may be due to the fact inhibition of mitochondrial activity, might alter the respiratory chain, generating a cytotoxic effect on the germ cell proliferation.41 It is further evidenced by an increased mid-piece defects and vacuolization in the mitochondria of the spermatozoa (Fig. 1.13). However, it's exact role is not defined.
Specialized Sperm Functional Assays
Hemizona Assay
The hemizona assay (HZA) measures the binding of capacitated sperm to isolated human zona pellucida. Human oocytes are bisected by micromanipulation, thus allowing for an internally controlled comparison of sperm binding (from patient versus a fertile control) to matching hemizona surfaces.
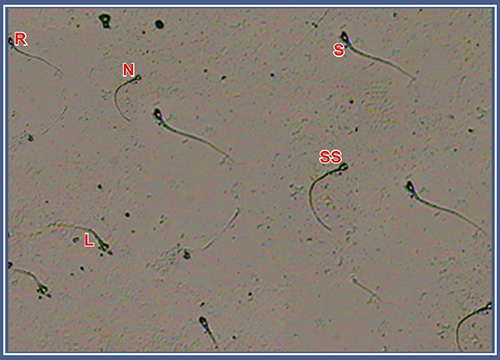
Fig. 1.13: Sperm mitochondrial activity index (SMAI)—Spermatozoa showing staining patterns on the mid-piece. S—standard, SS—substandard, L—low, R—residual, N—nil
The two matched hemizona of the human oocytes have the advantage of providing functionally equal surfaces allowing a controlled comparison of sperm binding and therefore limiting the amounts of oocytes used. Ethically this assay is acceptable since the microsurgical bisection of the oocyte prevents any inadvertent fertilization (Figs 1.14 and 1.15). The HZA has been found to be predictive of IVF outcome with positive and negative predictive values of 83% and 95% respectively.42 The major problem with this assay is the limited availability of human oocytes. Eventually it could be replaced by a standardized kit in which recombinant human zona sperm receptors mimic the natural functional hemizona used now.


Fig. 1.15: Hemizona assay: The spermatozoa showing varying degrees of fluorescence over the acrosomal region

Fig. 1.16: Zona-free hamster oocyte test: The zona-free hamster oocyte showing swollen heads indicating the penetration of spermatozoa
Sperm Penetration into Zona-free Hamster Oocytes
The zona-free hamster oocyte sperm penetration assay is a heterologous bioassay has originally been developed to test capacitation, acrosome reaction, fusion and sperm chromatin decondensation.43 Cross-species fertilization is made possible by removing the zona pellucida or hamster oocytes. Removal of the zona pellucida from hamster oocytes allows human sperm to fuse with hamster ova. This test is often termed as sperm penetration assay (SPA). For penetration to occur, sperm must undergo capacitation, the acrosome reaction, fusion with the oolemma and incorporation into the ooplasm. Using the original test conditions, the limiting step is the low incidence of spontaneous acrosome reaction in human sperm populations incubated in vitro, and therefore it has been described as measuring the ability of sperm to undergo acrosome reaction rather than the overall fertilization process (Fig. 1.16). Optimized procedures including acrosome reaction induction by ionophore A23187 are giving good predictive value of IVF and of incidence of pregnancy in the absence of treatment. Many versions of the SPA have been used clinically,20,46 and the value of the test results depends, in part, on the experience of the laboratory performing the assay.
Specialized tests on semen are not required for diagnosis of male infertility. They may be useful in a small number of patients for identifying a male factor contributing to unexplained infertility, or for selecting therapy, such as assisted reproductive technology.
Less Commonly used Specialized Tests
In addition to the zona-free hamster oocyte tests, numerous tests of sperm function have been employed in research studies. The acrosome reaction of human sperm can be detected26 using specialized staining techniques. Rates of spontaneous acrosome reactions and acrosome reactions induced by agents such as calcium ionophore and progesterone have been measured. Samples from infertile men tend to demonstrate higher spontaneous acrosome reaction levels and lower levels in the presence of inducers.47 In addition, sperm function can be evaluated using human zona pellucida binding tests. In some cases, these tests have detected a probable cause for low fertilization rates or failed IVF.48 A number of biochemical tests of sperm function have been studied. These include measurements of sperm creatine kinase49 and reactive oxygen species (ROS). ROS appear to be generated by both seminal leukocytes and sperm cells, and can interfere with sperm function by peroxidation of sperm lipid membranes and creation of toxic fatty acid peroxides.50,51
Less commonly used specialized tests on semen are important investigative tools, but are not necessary for the routine evaluation of men with infertility.
Various factors may be associated with variations in sperm characteristics among fertile individuals. These include increasing age, which is associated with diminution of semen volume, sperm motility and sperm morphology.52,53 A meta-analysis study has demonstrated that smokers present an average reduction of 13% in sperm concentration, 10% in sperm motility and 3% in sperm morphology.54 Seasonal variations in sperm quality, with greater concentration, motility and morphology in winter than in summer, have also been reported.55 The length of sexual abstinence preceding the collection of sperm for analysis is an important variable for the quality of the test. Very short or very long periods of abstinence are associated with distorted semen analysis results (WHO, 1999).20 Individuals who drink coffee everyday present increased sperm motility, although they present no significant alterations in the concentration or morphology of the sperm.56
CLINICAL IMPLICATIONS OF SEMEN ANALYSIS
Semen analysis is one of the most important diagnostic methods for the assessment of male infertility. The methodology for semen analysis has been undergoing constant improvement, and new assessment criteria have been proposed.4 Similarly, the reference values for each parameter have been the subject of debate. Modifications in sperm quality over the years have been reported and there has apparently been a decline, especially in sperm concentration.57,58 Regional differences in sperm parameters have frequently come to light.59,60 However, there are certain established variables which affect the seminal parameters.
Age
Various studies using animal models have reported reductions in fertility as age increases. Mice over 18 months of age undergo structural alterations in their germinative cells, with27 significant reduction in their numbers. Mice aged more than 33 months present an almost total cessation of spermatogenesis.61 Testicular atrophy and degeneration of the semniferous epithelium has been observed in rats of advanced age.62
In human beings, there is an association between aging and functional decline in the Leydig cells.63 Smaller semen volumes and lower sperm motility have been found to accompany advancing age among fertile individuals.64 There does not, however, appear to be any reduction in sperm concentration in elderly individuals.65 In contrast with the feminine menopause, which is accompanied by a reduction in fertility from the age of 35 years onwards, men may maintain their fertility into advanced old age. One birth of a child to a father aged 70 or over occurs for every 10,000 births of children to fathers aged 30 years.66 A large proportion of the individuals who seek assistance in infertility clinics are aged over 65.67
The data produced by the present study demonstrate a reduction in semen volume, sperm progressive motility and sperm normal morphology percentage from the age of 45 years onwards, as already described.64,65 The sperm concentration was lower in patients over 45 years of age, but this difference was not statistically significant (Table 1.4). However, since the majority of the sample for our study consisted of young individuals seeking sterilization by vasectomy, the effect of age on sperm concentration could not be exhaustively assessed.
|
Length of Sexual Abstinence
In fertile individuals, the length of sexual abstinence affects all semen parameters. With abstinence, there is increasing sperm concentration accompanied, however, by decreasing progressive motility and normal morphology percentage.68 Similar results have been observed among infertile patients, for whom a prolonged period of sexual abstinence was associated with increased semen volume ejaculated and increased sperm concentration, but with no reduction in progressive motility or normal morphology percentage (Table 1.5).6928
|
In particular situations, with the use of assisted reproduction techniques for infertile patients, prolonged sexual abstinence may be used for the purpose of obtaining a larger number of spermatozoa. Among 50 individuals with nonobstructive azoospermia who were candidates for testicular biopsy and ICSI into the oocyte, there was an increase in the total number of spermatozoa, although with no change in progressive motility when the period of abstinence was increased from 4 to 14 days.70
Seasonal Variation
Seasonal variation in conception rates for human beings has been described, with a reduction in the number of births in the spring as a consequence of a lower conception rate during the summer.71 Semen donors have not been found to have any seasonal alteration in sperm motility (Table 1.6). However, their sperm concentration has been found to be lower in the summer than in the winter.72
|
Individuals assessed for infertility have presented lower sperm concentration and progressive motility during the summer, with an improvement in these parameters over the winter months.73 Lower sperm motility and higher rates of sperm tail defects and immature forms were discovered during the summer months in 2,065 fertile men.74 Initially, the variations in semen parameters during the year were attributed to climatic differences. Thus, the high temperatures registered in the summer months were held responsible for the reduction in sperm quality, while it was thought that the low temperatures of the winter months would favor spermatogenesis.75,76 However, subsequent studies suggested that temperature was not the only factor involved and that the length of daylight also needed to be considered.77,78
Most of the studies have been conducted in countries of the northern hemisphere with large differences in climatic conditions between summer and winter. In Singapore, a tropical country in which the climatic differences are smaller, no differences in semen parameters in relation to the months of the year were found for 7,656 sperm analyses.79
Smoking
Despite the anti-smoking campaigns carried out throughout the world, the smoking habit is still quite common, affecting 35% of all adult European men65 and 33% of the individuals that we studied.80
The association between smoking and infertility has already been described, and reductions in sperm concentration, motility and normal morphology percentage among infertile patients who smoke have been observed.81,82 In a meta-analysis covering 27 studies on sperm quality among smokers, an average reduction of 13% in sperm concentration, 10% in motility and 3% in normal morphology percentage was observed (Table 1.7).83 The mechanism whereby smoking leads to infertility has still to be clarified. Hormone alterations are present in smokers, with an accompanying reduction in testosterone and an increase in the estradiol concentration in the blood.84 Genetic alterations in spermatozoa have also been described, since cigarettes contain more than 30 known mutagenic or carcinogenic chemical agents.85 However, the effects of cigarettes on common sperm parameters (concentration, motility and morphology) are still the subject of discussion and no study has yet been able to demonstrate clear evidence of a dose-response association. It is important to bear in mind that, in the majority of cases, smoking is just one aspect of a lifestyle that may include the consumption of alcohol, illegal medications or drugs, stress, dietary modifications and other factors that may have synergic or independent effects on sperm quality.30
|
|
The multiplicity of variables leads to methodological problems that hinder the clear establishment of what impact smoking has on the fertility of the male population as a whole.
Caffeine Intake
Studies using animal models have suggested that caffeine, when added to the sperm, may increase the motility of the spermatozoa.86,87 However, in humans, the results are still inconclusive, mainly because of the difficulty of quantifying the daily consumption of caffeine, in view of the fact that various foodstuffs contain this substance (for example chocolate and bottled soft drinks). Another important question is the stratification or control of other variables that may increase or decrease sperm motility and thus make it difficult to establish precisely the way in which caffeine affects sperm characteristics (Table 1.8).86
Keeping these variables in mind it is necessary to have a scientific approach to manage male infertility. Treatment of infertility involves comprehensive evaluation of both male and female to find an ideal solution to the couple's problem.31

Check Clinical History
The history and physical examination of the infertile man should be directed toward detection of factors associated with impaired fertility in men. After delineation of primary or secondary infertility for the man, a careful sexual history should be obtained, to confirm that the couple is having sexual intercourse with timing consistent with the achievement of conception. An understanding of the menstrual cycle and the importance of appropriate frequency of intercourse, without use of anti-sperm agents such as lubricants and avoidance of douching after intercourse, are important for the couple. Brief assessment of the infertility evaluation of the female partner should be obtained so that inappropriate intervention is32 not entertained for the man when fertility is not possible for the couple because of an irreparable female factor.
A history directed toward the general physical health of the man should then be performed, with specific attention to factors that impair male fertility potential. Specific childhood illnesses associated with infertility include cryptorchidism and post-pubertal mumps orchitis. The timing of pubertal landmarks and characteristics of secondary sexual development should be noted (onset of axillary and pubic hair, start of shaving, density of beard relative to male siblings). Operative intervention on the bladder neck (including Y-V plasty for UTI or vesicoureteral reflux) may be associated with retrograde ejaculation. Retroperitoneal Iymph node dissection for testis tumor and other retroperitoneal surgery may disrupt sympathetic pathways necessary for emission and antegrade ejaculation. Oral sympathomimetic drugs may allow the return of emission or conversion of retrograde to antegrade ejaculation in up to 50% of patients. Other men may be successfully treated with electroejaculation, if irreversible testicular dysfunction is not present.
Medical conditions such as diabetes or hypertension may affect sexual performance or testicular function. Diabetes can affect the sympathetic action necessary for bladder neck closure and antegrade ejaculation. Again, sympathomimetic drugs or electroejaculation may be used for treatment of these patients. Any generalized constitutional insult causing fever or viremia may impair testicular function. The effects of this insult can be detectable for up to 1 to 3 months after the infection.
Medications may also impair testicular or sexual function. A detailed history of all medications is needed to assess their potential effect on fertility. Sulfasalazine, cimetidine and nitrofurantoin have all been documented to impair testicular function for some men. Although antibiotics are necessary to treat infections that result in pyospermia and adversely affect fertility potential, long-term treatment of men with some antibiotics may also impair fertility, at least during the period of treatment. Androgenic drugs, such as anabolic steroids, can inhibit function of the hypothalamic-pituitary-testicular axis, leading to hypogonadism. Other drugs, including alcohol, nicotine and marijuana may adversely affect testicular function, directly or indirectly.
Physical Examination
Physical examination of the infertile man should be complete and thorough, since any significant medical condition may adversely affect testicular function.
Specific attention to the genitourinary examination is necessary. The penis should be evaluated for lesions, curvature and Peyronie's plaques. Location of the urethral meatus should be noted, and assessed relative to the ability of the patient to place the ejaculate33 deep within the vagina during intercourse for hypospadiac men. The abdomen should be palpated for abdominal masses and the inguinal regions closely inspected for scars.
The scrotal exam is most easily performed in a warm room. Initially the patient is examined supine. This causes varicocele if present, to collapse. The consistency of the testis can be best evaluated in this position, including the presence of any testicular masses. Testicular examination should carefully assess the volume and consistency of the testis, since the testicular volume is predominantly composed of seminiferous tubules. Testis tumors are often associated with excessive aromatase activity and infertility. Induration of the epididymis may be associated with inflammation and epididymal obstruction. Post-epididymal obstruction of the reproductive tract may result in fullness of the epididymis, when examined by an experienced physician. If clinically indicated a scrotal ultrasound should be performed to define the intratesticular and paratesticular structures.
The presence of the vasa deferentia should be confirmed bilaterally by palpation. Vascular engorgement of the spermatic cords should be assessed and the size of varicocele recorded. Large bilateral varicocele or a varicocele that does not decompress with the patient supine may suggest a fixed obstruction in the retroperitoneum and should be further evaluated with Doppler ultrasonography. Hernias in the inguinal region should also be assessed. Rectal examination should be performed to assess for prostatic irregularities, bogginess or tenderness. If clinically indicated a transrectal ultrasound examination should be performed to evaluate the prostate, seminal vesicles and ejaculatory ducts.
The results of history and physical examination are carry out before any additional tests to be ordered. However, the most critical component is the semen analysis report, which has the following vital components.
- Volume
- Sperm concentration per ml and for the total ejaculate
- Motility assessment with different grades
- Morphology assessment
- Vitality – the number of live sperms
- Agglutination and
- WBC, RBC with additional cells with fructose.
Define the Problem
If all these parameters are carefully looked into, with clear understanding of their reference ranges, a diagnosis in a particular individual may be obvious. This categorization facilitates identification of the exact cause and consequently additional tests can be ordered, if needed. By identifying where the problem is, viz. volume, pH, concentration, motility, morphology,34 vitality, infections, etc (by categorizing where the problem as either an isolated parameter defect or as a multiple parameter defect) it is quite easy to arrive at a cause specific diagnosis in majority of instances. Ideally it helps to identify the problem (Table 1.9). This will also facilitate a diagnosis based on etiology viz pretesticular, testicular or post-testicular which will facilitate a proper management plan.
Once the problem is identified, it is defined by using the following terminologies, which does not always indicate the degree or extent of the problem.
Definitions of “Abnormal” Counts
• Polyzoospermia | Excessively high sperm concentration |
• Hypospermia | Semen volume < 1.5 ml |
• Hyperspermia | Semen volume > 5.5 ml |
• Aspermia | No semen volume |
• Pyospermia | Leukocytes (germ fighter cells) present in semen |
• Hematospermia | Red blood cells present in semen |
• Necrozoospermia | Nonviable (“dead”) sperm |
COMPUTER-AIDED SPERM ANALYSIS—CASA
Computer-aided sperm analysis (CASA) requires sophisticated instruments for quantitative assessment of sperm from a microscopic image or from videotape. In principle, CASA can be used, to objectively measure sperm numbers, motility and morphology. CASA instruments are most useful clinically for assessing sperm motility and motion parameters, such as velocity or speed and head movement, which some believe may be important factors in determining sperm fertility potential.
|
Basic Instrumentation
In all CASA analyses, the user must verify that all motile spermatozoa in the field of view are being tracked. When used for kinematic analysis of non-capacitated spermatozoa in seminal plasma, the magnification of the CASA instrument should be such that the majority of spermatozoa are tracked for 0.5 seconds before leaving the field of view. Hence, for human spermatozoa minimum field of view should be no less than 200 × 200 µ minutes and also it should allow optimal tracking of spermatozoa with straight line velocity values up to 100 µ mt/s.
For human spermatozoa, an objective with maximum × 10 magnification and suitable numerical aperture must be used so as to provide an adequate depth of focus. For motility analysis, the digitizer should have maximum resolution consistent with standard video technology. Reliable analysis of human sperm motility ideally requires a minimum acquisition frequency of 50 Hz.88
Determination of Sperm Concentration
This must not be a primary reason for acquiring a CASA instrument. If a user wishes to use a CASA instrument to determine sperm concentration then he/she must establish that the intended measurement procedure provides accurate results compared with established, reliable techniques (e.g. WHO hemocytometry method and perhaps flow cytometry; WHO, 1992).19
It is considered that the current generation of CASA instruments does not provide accurate, reproducible values for sperm concentration unless the method can differentiate spermatozoa from other cells and debris by a specific staining method, e.g. fluorescent staining of DNA with quantitative determination of nucleus size.89
Determination of the Proportion of Motile Spermatozoa
This should not be considered a primary reason for acquiring a CASA instrument. If used in the routine analysis of seminal spermatozoa (Fig. 1.17), CASA should be used to determine the concentration of progressively motile spermatozoa. CASA can determine this value accurately if care is taken with specimen preparation, instrument use and appropriate user-defined criteria.90 Current CASA instruments should not be used for the determination of the proportion of motile spermatozoa, since they cannot be relied upon to distinguish between debris and dead spermatozoa while tracking live spermatozoa at the same time.36


Fig 1.18: Clinical application of CASA—The semen sample loaded on to the slide in the CASA instrument
Determination of Sperm Movement
For the time being, it is agreed that:91 (i) semen samples with sperm concentrations higher than those recommended by the CASA instrument manufacturer must be diluted using cell free autologous seminal plasma; (ii) all CASA analyses should be performed at body temperature (37°C for human spermatozoa); (iii) a minimum chamber depth of 10 mm must be used. Depths .20 mm are unlikely to be of any benefit; and (iv) at least 200 motile spermatozoa should be analyzed per sample (Fig. 1.18).37
Clinical Application of CASA
In the context of male fertility diagnosis, CASA should not be used without first undertaking a proper clinical assessment of the patient91 (including a clinical history and physical examination). For the present, CASA should not be undertaken in a clinical setting without first having constructed a basic semen profile according to recognized (WHO) guidelines.91
REFERENCES
- Thonneau P, Marchand S, Tallec A, et al. Incidence and main causes of infertility in a resident population (1,850,000) of three French regions (1988-1989). Hum Reprod 1991;6:811–6.
- Hull, et al. Br Med J 291, 1693-1697 (1985). Population study of causes, treatment, and outcome of infertility and Hull, MGR, Eddowes, HA, Fahy, U et al. Expectations of assisted conception for infertility. Br Med J 1992;304:1465–9.
- Jarow, Jonathan P Sharlip, ira d. +; belker, arnold m. ++; lipshultz, larry i. [s]; sigman, mark [//]; thomas, anthony j.; schlegel, peter n. [p]; howards, stuart s.; nehra, ajay**; damewood, marian d. ++; overstreet, james w.; sadovsky, richard; for the male infertility best practice policy committee of the american urological association inc. Best Practice Policies for Male Infertility. Journal of Urology 2002;167(5):2138–44.
- Report on the optimal evaluation of the infertile male. Fertility and sterility vol. 82,suppl. 1, september 2004, ISBN 0–9649702-1-5 (Volume 4) ISBN 09649702-6-0 (4 Volume set); An AUA Best Practice Policy and ASRM Practice Committee Report
- Jequier AM. Edward Martin (1859–1938) The founding father of modern clinical andrology. Int J Androl 1991;14:1–10.[ISI][Medline]
- MacLeod J. Human semen. Fertil Steril 1956;7:368–86.[ISI][Medline]
- MacLeod J. Seminal cytology in the presence of varicocele. Fertil Steril 1965;6:735–57.
- Jequier AM, Ukombe EB. Errors in the performance of a semen analysis. Br J Urol 1983;55:434–6.[ISI][Medline]
- Mortimer D, Templeton, AA, Lenton, EA, Coleman, RA. Semen analysis parameters and their interrelationships in suspected infertile men. Arch Androl 1982;8:165–71.[ISI][Medline]
- Mortimer D, Shu, MA, Tan, R. Standardization and quality control of sperm concentration and sperm motility counts in semen analysis. Hum Reprod 1986;1:299–303.[Abstract]
- Bjorndahl L, Barrett, CL, Fraser, LR, Kvist, U, Mortimer, D. ESHRE basic semen analysis courses 1995-1999: immediate beneficial effects of standardized training. Hum Reprod 2002;17:1299–1305.[Abstract/Free Full Text]
- Arumugam K. Sperm dysfunction in partners of infertile patients with minimal or mild endometriosis. Clin Exp Obstet Gynaecol 1993;20:43–7.
- Hammond MG, Jordan, S, Sloan, CS. Factors affecting pregnancy rates in a donor insemination program using frozen semen. Am J Obstet Gynecol 1986;155:480–5.[ISI][Medline]
- Kenemans P, Hafez, ES. Clinical application of scanning electron microscopy in human reproduction. Scanning Electron Microscopy 1984;1:215–42.
- Katz DF, Mills, RN, Pritchett, TR. The movement of human spermatozoa in cervical mucus. J Reprod Fertil 1982;53:259–65.
- World Health Organization. WHO laboratory manual for the examination of human semen and semen-cervical mucus interaction. Singapore: Press Concern; 1980.
- World Health Organization. WHO laboratory manual for the examination of human semen and semen-cervical mucus interaction. 2nd ed. Cambridge: Cambridge University Press, 1987.
- World Health Organization. WHO laboratory manual for the examination of human semen and semen-cervical mucus interaction. 3rd ed. Cambridge: Cambridge University Press, 1992.
- World Health Organization. WHO laboratory manual for the examination of human semen and semen-cervical mucus interaction. 4th ed. Cambridge: Cambridge University Press, 1999.
- Moutel G, Christian-Herve, Adnet JJ. Has traditional sperm analysis lost its clinical relevance? Fertil Steril 1997;67(3): 583–4; author reply 584-5. [Medline]
- Lemcke B, Behre, HM, Nieschlag, E. Frequently subnormal semen profiles of normal volunteers recruited over 17 years. Int J Androl 1997;20(3): 144–52. [Medline]
- Kruger TF, Acosta, AA, Simmons, KF, et al. Predictive value of abnormal sperm morphology in in vitro fertilization. Fertil Steril 1988;49:112–7. CLIA website: www.hcfa.gov/medicaid/clia/cliahome.Htm 5.
- Menkveld R, Wong, WY, Lombard, CJ, et al. Semen parameters, including WHO and strict criteria morphology, in a fertile and subfertile population: An effort towards standardization of in-vivo thresholds. Hum Reprod 2001;16(6): 1165–71. [Medline]
- Menkveld R, Stander, FS, Kotze, TJ, Kruger, TF, van Zyl JA. The evaluation of morphological characteristics of human spermatozoa according to stricter criteria. Hum Reprod 1990;5:586–92.
- Coetzee K, Kruger, TF, Lombard, CJ. Predictive value of normal sperm morphology: A structured literature review. Hum Reprod Update. 1998;4(1): 73–82. [Medline]
- Craig Niederberger. Complete Asthenospermia: To diagnose or not to diagnose?, Division of Andrology, University of Illinois, Chicago, Illinois. Journal of Andrology, Vol. 26,No. 3, May/June 2005
- Nathalie Rives, Nathalie Mousset-Simeon, Sophie Mazurier, Bertrand Mace. Primary flagellar abnormality is associated with an increased rate of spermatozoa aneuploidy. J Androl 2005;26: 61–69.
- Regina M Turner. Tales From the Tail: What do we really know about sperm motility? J Androl 2003;24:790–803.
- Kruger TF, Coetzee K. The role of sperm morphology in assisted reproduction. Hum Reprod Update 1999;5(2):172–8.
- Menkveld R, Kruger, TF. Advantages of strict (Tygerberg) criteria for evaluation of sperm morphology. Int J Androl 1995;18(Suppl 2): 36–42.
- Van Waart J, Kruger TF, Lombard CJ, Ombelet W. Predictive value of normal sperm morphology in intrauterine insemination (IUI): A structured literature review. Hum Reprod Update 2001;7(5): 495–500.
- Marchini M, Ruspa M, Baglioni A, Piffaretti-Yanez A, Campana A, Balerna M. Poor reproductive prognosis in severe teratozoospermia with a predominant sperm anomaly. Journal 1989;21(5): 468–75.
- Wolff H, Anderson, DJ. Immunohistologic characterization and quantitation of leukocyte subpopulations in human semen. Fertil Steril 1988;49:497–504.
- Ayvaliotis B, Bronson, R, Rosenfeld, D, Cooper, G. Conception rates in couples where autoimmunity to sperm is detected. Fertil Steril 1985;43:739–42.
- Chan SY, Wang, C, Chan, ST, Ho, PC. Department of Obstetrics and Gynaecology, University of Hong Kong, Differential evaluation of human sperm hypo-osmotic swelling test and its relationship with the outcome of in-vitro fertilization of human oocytes. Human Reproduction 1984;5:84–88.
- Tambe AS, Kaore, SB, Sawane, MV, Gosavi, GB. Acrosome intactness and seminal hyaluronidase activity: Relationship with conventional seminal parameters. Indian J Med Sci 2001;55(3):125–32.
- Huret JL. Nuclear chromatin decondensation of human sperm: A review. Archives of Andrology 1986;16:97–109.
- Reyes R, Rosado, A, Hernandez, O, Delgado, NM. Heparin and glutathione: Physiological decondensing agents of human sperm nuclei. Gamete Research 1989;23:39–47.
- Kim IC, Waller, DP. Specific inhibition of the testicular mitochondrial respiratory chain in vitro by gossypol. J Androl 1984;5:424–30. Lohiya NK et al. Asian J Androl 2002;4 (1): 17–26.
- Yogev L, Homonnai, ZT, Gamzu, R, Amit, A, Lessing, JB, Paz, G, Yavetz, H. The use of hemizona assay in the evaluation of the optimal sperm preparation technique, Institute for the Study of Fertility, Serlin Maternity Hospital, Tel Aviv Sourasky Medical Center, Israel. Human Reproduction 1995;10:851–4.
- Barros C, Gonzalez, J, Herrera, E, Bustos-Obregon E. Human sperm penetration into zona-free hamster oocytes as a test to evaluate the sperm fertilizing ability. Andrologia 1979;11(3):197–210.
- Oei SG, Helmerhorst, FM, Bloemenkamp, KM, Hollants, FM, Meerpoel, DE, Keirse, JNC. Effectiveness of the postcoital test: randomised controlled trial. BMJ 1998;317:502–5.
- Glatstein IZ, Harlow, BL, Hornstein, MD. Practice patterns among reproductive endocrinologists: Further aspects of the infertility evaluation. Fertil Steril 1998;70:263–9.
- Smith RG, Johnson, A, Lamb, D, Lipshultz, LI. Functional tests of spermatozoa. Sperm penetration assay. Urol Clin North Am 1987;14:451–8.
- Brucker C, Lipford, GB. The human sperm acrosome reaction: Physiology and regulatory mechanisms. An update. Human Reproduction Update, 1995;1(1):51–62.
- Yanagimachi R, Yanagiimachi, H, Rogers, BJ. The use of zona-free animal ova as a test system for the assessment of the fertilizing capacity of human spermatozoa. Biol Reprod 1976;15:471–6.[Medline]
- Gergely A, et al. Sperm creatine kinase activity in normospermic and oligozoospermic Hungarian men. J Assist Reprod Genet 1999;16(1):35–40.
- Griveau JF, Le Lannou D, et al. Reactive oxygen species and human spermatozoa: Physiology and pathology. Int J Androl 1997;20(2): 61–9. PMID: 9292315.
- Jiøí Novotnýa. The Occurrence of Reactive Oxygen Species. In The Semen of Males from Infertile Couples; Biomed Papers 2003;147(2):173–6.
- Lemcke B, Behre, HM, Nieschlag, E. Frequently subnormal semen profiles of normal volunteers recruited over 17 years. Int J Androl 1997;20(3): 144–52. [Medline]
- Spandorfer SD, Avrech, OM, Colombero, LT, Palermo, GD, Rosenwaks, Z. Effect of parental age on fertilization and pregnancy characteristics in couples treated by intracytoplasmic sperm injection. Hum Reprod 1998;13(2): 334–8. [Medline]
- Vine MF. Smoking and male reproduction: A review. Int J Androl 1996;19(6): 323–37. [Medline]
- Andolz P, Bielsa, MA, Andolz, A. Circannual variation in human semen parameters. Int J Androl 2001;24(5): 266–71. [Medline]
- Jensen TK, Henriksen, TB, Hjollund, NH, et al. Caffeine intake and fecundability: A follow-up study among 430 Danish couples planning their first pregnancy. Reprod Toxicol 1998;12(3):289–95.
- Irvine S, Cawood, E, Richardson, D, MacDonald E, Aitken J. Evidence of deteriorating semen quality in the United Kingdom: Birth cohort study in 577 men in Scotland over 11 years. BMJ 1996;312(7029): 467–71. [Medline]
- Jorgensen N, Andersen, AG, Eustache, F, et al. Regional differences in semen quality in Europe. Hum Reprod 2001;16(5): 1012–9.[Medline]
- Auger J, Jouannet P. Evidence for regional differences of semen quality among fertile French men. Federation Française des Centres d’Étude et de Conservation des Oeufs et du Sperme humains. Hum Reprod 1997;12(4): 740–5. [Medline]
- Tanemura K, Kurohmaru, M, Kuramoto, K, Hayashi, Y. Age-related morphological changes in the testis of the BDF1 mouse. J Vet Med Sci 1993;55(5): 703–10. [Medline]
- Parkening TA, Collins, TJ, Au, WW. Paternal age and its effects on reproduction in C57BL/6NNia mice. J Gerontol 1988;43(3):B79–84. [Medline]
- Gray A, Feldman, HA, McKinlay JB, Longcope C. Age, disease, and changing sex hormone levels in middle-aged men: Results of the Massachusetts Male Aging Study. J Clin Endocrinol Metab 1991;73(5): 1016–25. [Medline]
- Eskenazi B, Wyrobek, AJ, Sloter, E, et al. The association of age and semen quality in healthy men. Hum Reprod 2003;18(2): 447–54. [Medline]
- Kidd SA, Eskenazi, B, Wyrobek, AJ. Effects of male age on semen quality and fertility: A review of the literature. Fertil Steril 2001;75(2): 237–48. [Medline]
- Rolf C, Behre, HM, Nieschlag, E. Reproductive parameters of older compared to younger men of infertile couples. Int J Androl 1996;19(3): 135–42. [Medline]
- Plas E, Berger, P, Hermann, M, Pfluger, H. Effects of aging on male fertility? Exp Gerontol 2000;35(5): 543–51. [Medline]
- Pellestor F, Girardet, A, Andreo, B. Effect of long abstinence periods on human sperm quality. Int J Fertil Menopausal Stud 1994;39(5): 278–82. [Medline]
- Mortimer D, Templeton, AA, Lenton, EA, Coleman, RA. Influence of abstinence and ejaculation-to-analysis delay on semen analysis parameters of suspected infertile men. Arch Androl 1982;8(4): 251–6. [Medline]
- Raziel A, Friedler, S, Schachter, M, et al. Influence of a short or long abstinence period on semen parameters in the ejaculate of patients with nonobstructive azoospermia. Fertil Steril 2001;76(3): 485–90. [Medline]
- Krause A, Krause W. Seasonal variations in human seminal parameters. Eur J Obstet Gynecol Reprod Biol 2002;101(2): 175–8. [Medline]
- Saint Pol P, Beuscart R, Leroy-Martin B, Hermand E, Jablonski W. Circannual rhythms of sperm parameters of fertile men. Fertil Steril 1989;51(6): 1030–3. [Medline]
- Schalue TK, Webert, SK, Rognsvoog, LM, et al. Monthly variation among semen samples from 4114 infertility patients. Cincinnati: Annual Meeting of the American Society for Reproductive Medicine, 1997.
- Centola GM, Eberly S. Seasonal variations and age-related changes in human sperm count, motility, motion parameters, morphology, and white blood cell concentration. Fertil Steril 1999;72(5): 803–8. [Medline]
- Levine RJ, Bordson, BL, Mathew, RM, Brown, MH, Stanley, JM, Star, TB. Deterioration of semen quality during summer in New Orleans. Fertil Steril 1988;49(5): 900–7. [Medline]
- Politoff L, Birkhauser, M, Almendral, A, Zorn, A. New data confirming a circannual rhythm in spermatogenesis. Fertil Steril 1989;52(3): 486–9. [Medline]
- Levine RJ, Brown, MH, Bell, M, Shue, F, Greenberg, GN, Bordson, BL. Air-conditioned environments do not prevent deterioration of human semen quality during the summer. Fertil Steril 1992;57(5): 1075–83. [Medline]
- Chia SE, Lim, ST, Ho, LM, Tay, SK. Monthly variation in human semen quality in male partners of infertile women in the tropics. Hum Reprod 2001;16(2): 277–81. [Medline]
- Trummer H, Habermann, H, Haas, J, Pummer, K. The impact of cigarette smoking on human semen parameters and hormones. Hum Reprod 2002;17(6): 1554–9. [Medline]
- Apresentação OPAS. 1° Congresso Internacional de Prevenção de Tabagismo, Belo Horizonte, Minas Gerais; 2002.
- Sofikitis N, Miyagawa, I, Dimitriadis, D, Zavos, P, Sikka, S, Hellstrom, W. Effects of smoking on testicular function, semen quality and sperm fertilizing capacity. J Urol 1995;154(3): 1030–4. [Medline]
- Zinaman MJ, Brown, CC, Selevan, SG, Clegg, ED. Semen quality and human fertility: a prospective study with healthy couples. J Androl 2000;21(1): 145–53. [Medline]
- Vogt HJ, Heller, WD, Borelli, S. Sperm quality of healthy smokers, ex-smokers, and never-smokers. Fertil Steril 1986;45(1): 106–10. [Medline]
- Rubes J, Lowe, X, Moore D 2nd, Perreault S, et al. Smoking cigarettes is associated with increased sperm disomy in teenage men. Fertil Steril 1998;70(4): 715–23. [Medline]
- Maxwell WM, Robinson, SJ, Roca, J, Molinia, FC, Sanchez-Partida LG, Evans G. Motility, acrosome integrity and fertility of frozen ram spermatozoa treated with caffeine, pentoxifylline, cAMP, 2-deoxyadenosine and kallikrein. Reprod Fertil Dev 1995;7(5): 1081–7. [Medline]
- Stachecki JJ, Ginsburg, KA, Armant, DR. Stimulation of cryopreserved epididymal spermatozoa of the domestic cat using the motility stimulants caffeine, pentoxifylline, and 2’-deoxyadenosine. J Androl 1994;15(2): 157–64. [Medline]
- Mortimer D, Serres, C, Mortimer, ST, Jouannet, P. Influence of image sampling frequency on the perceived movement characteristics of capacitating human spermatozoa. Gamete Res 1988;20:313–27.
- Zinaman MJ, Uhler, ML, Vertuno, E, et al. Evaluation of computer assisted semen analysis (CASA) with IDENT stain to determine sperm concentration. J Androl 1996;17:288–92.
- Mortimer D, Aitken, RJ, Mortimer, ST, Pacey, AA. Workshop report: Clinical CASA—the quest for consensus. Reprod Fertil Dev 1995;7:951–9.
- ESHRE Andrology Special Interest Group. Consensus workshop on advanced diagnostic andrology techniques. Hum Reprod 1996;11:1463–79.