

The ability to locate anatomical structures via the surface of the body using observation, palpation and reference landmarks is an essential part of clinical medicine. A sound knowledge of surface anatomy enables a practitioner to understand the basis of physical examinations and medical procedures such as cannulation, biopsy, surgical incisions, local anaesthesia and intra-articular injection. Surface anatomy also assists with diagnostic reasoning and in the interpretation of medical images; for example, much of the anatomy visible on a chest or abdominal X-ray can be deciphered from surface anatomy images.
Measurements and variability
The descriptions within this book are based upon current observations, evidence and practice and the authors’ own observations. Although the surface positions of many structures are relatively consistent, surface anatomy is subject to inter-individual variability and changes with body shape, size, condition, age and position. As well as helping redefine our knowledge of surface anatomy, recent imaging-based studies are providing insight into the normal ranges of positional variance. A selection of evidence-based studies are referenced on page x.
The measurements provided in this text should be used as a guide. A good practitioner needs to be aware of variability and should use observation, palpation, percussion, auscultation, nerve stimulation or ultrasound to further guide positioning. In certain areas finger-breadth measurements are used since they often provide a useful quick measurement; these start with the tip of the index finger.
Ultrasound and surface anatomy
Ultrasound provides additional guidance during diagnostic and invasive procedures and is a useful tool for learning 2surface anatomy because it permits the direct visualisation of anatomical structures in a given location. Ultrasound cannot replace the need to learn surface anatomy; to the contrary, a sound knowledge of the latter is fundamental to the correct placement of the probe and to image interpretation.
3
Palpation techniques
Efficient palpation technique is an essential element of clinical practice. It is used to localise anatomical structures and landmarks, and to determine tissue structure and pathological change. As a general rule sides are compared, especially when pathology is suspected. Tenderness should not normally be elicited upon palpation. Different techniques are used to palpate specific features, regions and tissues (Table 1.1), and many tissues have distinct characteristics:
- Bone feels hard and resists digital pressure
- Muscle, in contrast to bone, yields to digital pressure and both moves and changes shape upon contraction
- Tendons feel firm and cord-like: with a muscle relaxed its tendon can be moved perpendicular to its line of pull, and on muscle contraction the tendon can be felt to move and become more fixed in position
- Ligaments may feel firm and cordlike, or may be impalpable
- Nerves are generally impalpable, although some larger nerves (e.g. ulnar) may be felt as a soft cord-like structure that can be moved perpendicular to their course/direction
1.1 THE ANATOMICAL POSITION AND PLANES
The anatomical position
Within this book all positions, relationships and movements of body structures have been described in relation to the anatomical position. The anatomical position is the standard reference position of the body (Figure 1.1), in which a subject is standing upright with:
- Face, eyes, palms and toes facing forwards (anteriorly)
- Upper limbs by the sides of the body, fingers together
- Lower limbs, feet, fingers and toes together


Relative positional terms
From the starting point of the anatomical position it is possible to describe the relative positions of structures using a standardised set of terms (Figure 1.2 and Table 1.2).
Anatomical planes
From the anatomical position the body can be sectioned by three mutually perpendicular planes (Figure 1.3 and Table 1.3).5
|


|
1.2 ANATOMICAL MOVEMENTS
The movement of a joint or part of the body is described from the starting point of the anatomical position. A knowledge of joint movement is useful in surface anatomy since specified movements can aid structure identification and be required for clinical examination and procedures.
Flexion and extension
Flexion and extension occur in the sagittal plane (Figures 1.4–1.14).
8
9




Figure 1.7: Digital flexion and extension: (a) metacarpophalangeal (MCP) and interphalangeal (IP) joints; (b) metacarpophalangeal (MCP) joints.





Figure 1.12: Toe dorsiflexion (extension) and plantarflexion (flexion) at the metatarsophalangeal and interphalangeal joints.


- Flexion brings together two surfaces that were originally on the ventral surface of the embryo
- Extension moves apart two surfaces that were originally on the ventral surface of the embryo
Flexion moves most structures anteriorly whereas extension moves most structures posteriorly. The main exceptions to this occur at the knee, ankle, toes and thumb. For example, plantarflexion is the flexion movement of the feet or toes, dorsiflexion being the extension movement. Flexion of the thumb moves it across the palm in a coronal plane, and extension moves it in the opposite direction.
Abduction and adduction
Abduction and adduction occur in the coronal plane (Figures 1.15–1.20).
- Abduction moves a structure away from the median plane
- Adduction moves a structure closer to the median plane
The digits differ in that the movements take place in relation the 3rd digit in the hand and the 2nd digit in the foot. Abduction of the thumb moves it away from the palm in a sagittal plane, and adduction returns it to the anatomical position.12


Figure 1.16: Hip abduction and adduction. Hip adduction can take place across the midline if opposite limb is avoided.




Figure 1.20: Toe (a) abduction and (b) adduction relative to digit 2. The blue line (digit 2) represents the axis of abduction/adduction.



Rotation
Rotation occurs in the transverse plane (Figures 1.21–1.24).
- Medial (internal) rotation moves the anterior surface of a limb closer to the median plane
- Lateral (external) rotation moves the anterior surface of the limb away from the median plane

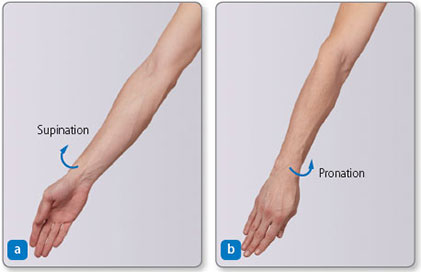
Figure 1.25: Forearm supination and pronation. (a) Supination brings to supine position. (b) Pronation brings forearm to prone position.
Pronation and supination
In the forearm:
- Pronation rotates the radius medially around the ulna such that the palm of the hand faces posteriorly (Figure 1.25)16
- Supination is the opposite movement: it returns the palm to the anatomical position


In the foot:
- Pronation lifts its lateral edge such that the sole face away from the median sagittal plane
- Supination lifts the medial edge such that the sole faces the median sagittal plane (Figure 1.26)
Foot pronation and supination is usually accompanied by foot abduction and adduction, respectively.
Inversion and eversion of the foot
- Inversion is a combination of adduction, supination and plantarflexion

Both movements occur naturally when attempting to make the sole face medially or laterally with the foot lifted off the floor.
Mandibular movements
- Protrusion moves the mandible (and therefore the chin) anteriorly in a transverse plane
- Retrusion moves the mandible posteriorly back to the anatomical position (Figure 1.28)
Mandibular opening combines protrusion and rotation.
Scapular movements
- Protraction moves the scapula anterolaterally around the thoracic wall, such as when reaching forward; retraction is the opposite posteromedial movement towards the vertebral column (Figure 1.29)
- Elevation moves the scapula superiorly on the thoracic wall, such as when shrugging the shoulder; depression is the opposite inferior movement (Figure 1.30)
- External/lateral rotation makes the glenoid fossa face superolaterally; internal/medial rotation is the opposite movement (Figure 1.31)18

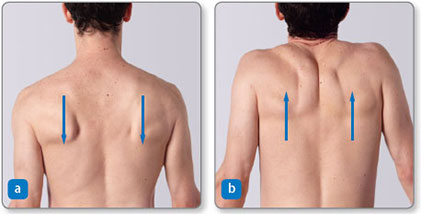

Figure 1.31: Scapular movements: (a) medial (internal) rotation and (b) lateral (external) rotation.
Opposition and reposition of the digits
- Opposition is the pad-to-pad contact of the thumb and fingers; it involves a specialised movement of the thumb (Figure 1.32) and is essential for fine dexterous activities such as writing and buttoning clothes
- Reposition returns the thumb to the anatomical position



Lateral flexion
Lateral flexion is a lateral movement of the vertebral column in a coronal plane, which results in the head moving away from the midline (median plane) (Figures 1.33 and 1.34).21

Figure 1.35: Eye movements. Ⓔ Elevation, Ⓓ depression, Ⓛ left-eye abduction and right-eye adduction, Ⓡ right-eye abduction and left-eye adduction.

Figure 1.36: Eye movement: convergence. (a) the neutral anatomical position and (b) convergence (with a mild depression)
Eye movements
The eyes move around three different mutually perpendicular axes. The movements of abduction–adduction, elevation–depression, and combinations of these are easily observed (Figure 1.35). Most eye movements are conjugate (i.e. both eyes move in the same direction, by the same amount and at the same time), except for convergence, in which both eyes adduct to enable observation of nearby objects (Figure 1.36).22
1.3 SENSORY INNERVATION
A knowledge of cutaneous innervation patterns is important when mapping out sensory losses because it provides clues as to the location of damage. Cutaneous innervation is defined by:
- Cutaneous (named peripheral) nerve areas (Figures 1.39 and 1.40) – the area of skin innervated by a peripheral cutaneous nerve (e.g. ulnar nerve); cutaneous nerve areas may cross parts of one or more dermatomes
As a general rule:
- Dermatomal sensory losses occur following damage to the spinal nerves or their ventral rami, or the spinal cord
- Cutaneous nerve area sensory losses occur as a result of nerve lesions in peripheral sites via surgical incisions, laceration or regional compression
- Superficial cutaneous nerves in the limbs often run close to superficial veins and are therefore vulnerable to injury during cannulation; similarly major peripheral nerves (e.g. femoral nerve) run close to arteries and are vulnerable during arterial access

Figure 1.37: An evidence-based pelvic dermatome map. Based on Lee MWL, McPhee RW, Stringer MD. An evidence-based approach to human dermatomes. Clin Anat 2008; 21:363–373.

Figure 1.38: An evidence-based dermatome map. Based on Lee MWL, McPhee RW, Stringer MD. An evidence-based approach to human dermatomes. Clin Anat 2008; 21:363–373.

